
Журнал «Травма» Том 15, №5, 2014
Вернуться к номеру
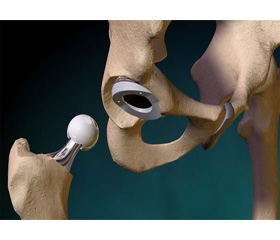
Features of hip replacement in severe types of dysplasia
Авторы: Poluliakh M., Gerasimenko S., Kostyuk A., Poluliakh D., Babko A., Gerasimenko A. - State Institution «Institute of traumatology and oprthopedics Academy of Medical Sciences of Ukraine»
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
dysplastic coxarthrosis, total arthroplasty.
Introduction
Dysplastic coxarthrosis is concerned to one of the most severe pathology of the hip joint, frequency of which compose from 21 up to 80 % of all diseases of the joints [9].
Dysplastic coxarthrosis has its own characteristics, which are caused by the young age of the patients, rapid progression of the disease and lower the effect of conservative treatment that extends the indications for hip replacement and is an urgent problem in modern orthopedics [13]. Hip arthroplasty in dysplastic coxarthrosis, especially in severe types is a difficult and high-tech surgery [7, 8].
The matter of putting acetabular component of the prosthesis relative to its anatomical position, the use of bone grafting of the acetabular roof, bringing down the thigh and reposition head of prosthesis remain the most relevant in hip arthroplasty in severe forms of dysplastic coxarthrosis.
The purpose of the study – to optimize the tactic of hip arthroplasty in severe types of dysplastic coxarthrosis.
Material and methods
The study is based on the analysis of total hip arthroplasty among patients with severe type of dysplasia (Crowe III, IV). There were 29 patients who underwent 38 hip joint arthroplasty. Nine patients underwent a hip arthroplasty on both sides. Most of the patients were women - 28, and one male patient. There were 28 cases of Crowe type III hip dysplasia and 10 cases of IV Crowe type dysplasia. The average age of patients was 44.2 years.
Results and discussion
The hip arthroplasty with one-stage lengthening limb was performed in dysplastic coxarthrosis Crowe III, IV types with shortened limbs up to 4 cm. When shortening of the limb is about 4-5 cm a one-stage limb lengthening is fraught with complications from the neurovascular bundle , moreover, is not always possible to perform reposition of the head of prosthesis, especially among patients who have already underwent thr surgery on the hip joint in childhood. Such patients underwent the shortening osteotomy of the proximal femur.
In cases where there is a need for lengthening a limb for more than 5 cm, the surgery was performed in two stages. On the first phase the rod devise of external fixation was imposed with the introduction to the bones of the pelvis and femur. The assembly of the rod of external fixation device allows a one-stage lengthening of a limb, performed during blending the device under general anesthesia, and then for a few days the lengthening of the limb have been continued, by this mean the femoral head has been brought up to the true acetabulum . After achieving the goal, the device was disassembled. And after the healing of the rods the hip arthroplasty was performed.
The treatment results among patients have been examined in the period from 6 months till 5 years.