Резюме
Актуальність. Визначення ендотеліальної функції за допомогою неінвазивних методів відіграє основну роль у прогнозуваннi перебігу різних захворювань, ризику розвитку ускладнень та оцінцi лікування. Мета: оцінка ендотеліальної функції в пацієнтів iз хронічними запальними захворюваннями кишечника (ХЗЗК) залежно від їхнього нутритивного статусу шляхом визначення стану судинного ендотелію в пробі з реактивною гіперемією та вмісту метаболітів оксиду азоту (МОА) в сироватці крові. Матеріали та методи. Сто двадцять пацієнтів iз ХЗЗК (81 — iз неспецифічним виразковим колітом (НВК) та 39 пацієнтів із хворобою Крона (ХК)) були розподілені на групи залежно від антропометричних характеристик: І — зі зниженим нутритивним статусом (n = 70); ІІ — iз нормальним (n = 20); ІІІ — iз підвищеним нутритивним статусом (n = 30). У сироватці крові пацієнтів вимірювали рівень МОА за В.А. Метельською. Для оцінки ендотеліальної функції визначали ендотелійзалежну вазодилатацію плечової артерії в пробі з реактивною гіперемією. Результати. На основі проведених досліджень встановлено вірогідне зниження вмісту МОА в сироватці крові: у пацієнтів iз НВК — у 1,7 раза (р < 0,01) та з ХК — в 1,9 раза (р < 0,001). Зниження вмісту МОА в сироватці крові не залежало від нутритивного статусу пацієнтів iз ХЗЗК. Порушення функції судинного ендотелію виявлено в 76,7 % випадків: зниження функції ендотелію — у 49,2 %, дисфункція — у 27,5 %. Зміни функції судинного ендотелію зареєстровано в 75,7 % пацієнтів І групи, 75 % — ІІ та у 83,4 % пацієнтів ІІІ групи, переважно внаслiдок зниження функції ендотелію. Висновки. Показано, що в 71 % пацієнтів iз ХЗЗК відбувається вірогідне зниження вмісту МОА в сироватці крові, що не залежить від їхнього нутритивного статусу. У хворих iз НВК спостерігалися більш виражені зміни у частотi виявлених порушень та більш значне зростання діаметра плечової артерії порівняно iз пацієнтами з ХК. Зниження нутритивного статусу супроводжувалося змінами функції судинного ендотелію в 75,4 % випадків.
Актуальность. Определение эндотелиальной функции с помощью неинвазивных методов играет основную роль в прогнозировании течения различных заболеваний, риска развития осложнений и оценке лечения. Цель: оценка эндотелиальной функции у пациентов с хроническими воспалительными заболеваниями кишечника (ХВЗК) в зависимости от их нутритивного статуса путем определения состояния сосудистого эндотелия в пробе с реактивной гиперемией и содержания метаболитов оксида азота (МОА). Материалы и методы. Сто двадцать пациентов с ХВЗК (81 — с неспецифическим язвенным колитом (НЯК) и 39 пациентов с болезнью Крона (БК)) были разделены на группы в зависимости от антропометрических характеристик: I — со сниженным нутритивным статусом (n = 70); II — с нормальным (n = 20); III — с повышенным нутритивным статусом (n = 30). В сыворотке крови пациентов измеряли уровень МОА по В.А. Метельской. Для оценки эндотелиальной функции определяли эндотелийзависимую вазодилатацию плечевой артерии в пробе с реактивной гиперемией. Результаты. На основе проведенных исследований установлено достоверное снижение содержания МОА в сыворотке крови: у пациентов с НЯК — в 1,7 раза (р < 0,01) и с ХК — в 1,9 раза (р < 0,001). Снижение содержания МОА в сыворотке крови не зависело от нутритивного статуса пациентов с ХВЗК. Нарушение функции сосудистого эндотелия обнаружено в 76,7 % случаев: снижение функции эндотелия — в 49,2 %, дисфункция — в 27,5 %. Изменения функции сосудистого эндотелия зарегистрированы у 75,7 % пациентов I группы, 75 % — II и у 83,4 % пациентов III группы, преимущественно вследствие снижения функции эндотелия. Выводы. Показано, что у 71 % пациентов с ХВЗК происходит достоверное уменьшение содержания МОА в сыворотке крови, что не зависит от их нутритивного статуса. У больных с НЯК наблюдались более выраженные изменения в частоте выявленных нарушений и более значительное увеличение диаметра плечевой артерии по сравнению с пациентами с БК. Снижение нутритивного статуса сопровождалось изменениями функции сосудистого эндотелия в 75,4 % случаев.
Background. Evaluation of endothelial function by non-invasive methods plays a major role in predicting the course of various diseases, the risk of complications and assessing the treatment. The purpose was to evaluate endothelial function in patients with chronic inflammatory bowel disease (IBD) according to their nutritional status by determining the state of vascular endothelium with reactive hyperemia test and the content of nitrogen oxide metabolites (NOx). Materials and methods. 120 chronic IBD patients (81 individuals with nonspecific ulcerative colitis (NUC) and 39 — with Crohn’s disease (CD)) were divided into groups depending on the anthropometric characteristics: I — reduced nutritional status (n = 70); II — normal nutritional status (n = 20); III — increased nutritional status (n = 30). In the blood serum of patients, the level of NOx was determined according to V.A. Metelskaya technique. To assess endothelial function, endothelium-dependent vasodilation of the brachial artery was determined by reactive hyperemia test. Results. Based on conducted studies, a significant decrease in the NOx serum content was observed: 1.7-fold (p < 0.01) — in NUC patients and 1.9-fold (p < 0.001) — in BD patients. Reduction of the NOx content in the blood serum did not depend on the nutritional status of individuals with chronic IBD. Violation of vascular endothelial function was found in 76.7 % of cases: decreased endothelial function — in 49.2 %, endothelial dysfunction — in 27.5 %. Changes in vascular endothelial function were found in 75.7 % of group I patients, 75 % of group II and 83.4 % of group III patients, mainly due to decreased endothelial function. Conclusions. It is shown that 71 % of chronic IBD patients have a significant decrease in serum NOx, which does not depend on their nutritional status. Patients with NUC have more significant changes in the incidence of detected disorders and more pronounced increase in the diameter of the brachial artery compared with CD patients. Reduced nutritional status was accompanied with the changes in vascular endothelial function in 75.4 % of cases.
Introduction
Inflammatory bowel diseases (IBD), including nonspecific ulcerative colitis (NUC) and Crohn’s disease (CD), lead to chronic inflammation, mainly affecting the gastrointestinal tract. This pathology requires surgical intervention in 16 and 47 % of NUC and CD patients, respectively, every 10 years after the onset of the disease. As a result, patients with chronic IBD experience a significant decline in the quality of life, compared to healthy people of the same age [1]. According to recent epidemiological studies, the annual incidence of NUC in Europe is 10.4, and CD — 5.6 cases per 100,000 population, with the largest gradient observed in Scandinavia (24.5 and 9.2 cases per 100,000, respectively). In Europe, more than 2.2 million people suffer from these diseases. NUC is being detected somewhat more often in men than in women — 1.39 : 1, whereas with CD, the opposite ratio is determined — 1 : 1.12 [2].
In Ukraine in 2015, intestinal diseases accounted for 3.7 % in the structure of digestive diseases, with a predominance of NUC over CD (4.4 : 1). Aside from that, it is important to note that the absolute number of CD among the working-age population has increased [3].
Endothelial dysfunction is a multifaceted process, one of the earliest manifestations of which is violation of nitric oxide (NO) bioavailability under the influence of many pathological factors [4]. NO belongs to the most important biological mediators in the human body and participates in the regulation of intra- and intercellular processes in various organs and tissues. Its serum content depends on many factors: the activity of NO synthase, structural and functional state of the endothelium, concentration of free radicals, exo- and endotoxins, inflammatory mediators, etc. [5]. Oxidative stress is the cause of nitrite and nitrate inactivation and, accordingly, leads to a decrease in the concentration of NO in the tissues, preventing vasodilation. Insufficient production of endothelial NO is associated with increased tone and vascular spasm, increased vascular permeability for proteins and lipoproteins, accelerated proliferation of smooth muscle cells, expression of adhesive molecules on the surface of endothelial cells without interference, increased thrombus formation [6]. Various pathological processes in the body are accompanied by vascular endothelium dysfunction, which may lead to the progression of vascular insufficiency. The evaluation of endothelial function by non-invasive methods plays a major role in predicting disease course, the risk of complications, and assessing the treatment [7, 8].
Methods for studying the endothelial function can be divided into two large groups: I — invasive techniques, in which instrumental, clinical and laboratory methods are used; II — non-invasive options based on the methods of functional diagnosis. The golden standard for the study of endothelial function is currently not established yet [9]. Over the past 25 years, many methodological approaches have been developed to evaluate the endothelial function in humans [10]. Possibilities of measuring indicators that characterize the endothelial function are widely used in scientific studies. However, their use as a clinical tool in daily medical practice is still not common [11].
The purpose of the present work was to assess the endothelial function in patients with chronic inflammatory bowel disease according to their nutritional status by determining the state of vascular endothelium by reactive hyperemia test and the content of nitrogen oxide metabolites (NOx).
Materials and methods
120 chronic IBD patients (81 patients with NUC and 39 — with CD) were examined at the department of bowel diseases of the Institute of Gastroenterology of the National Academy of Medical Sciences of Ukraine during 2014–2016; among them 45.8 % of women, 54.2 % of men with the mean age of (38.13 ± 1.08) years. Depending on the anthropometric characteristics, all patients were divided into three groups: I — with reduced nutritional status (n = 70); ІІ — with normal nutritional status (n = 20); III — with increased nutritional status (n = 30).
Patients’ blood serum was used to determine the level of NOx according to V.A. Metelskaya technique, where vanadium chloride (Sigma-Aldrich) was used as a reducing agent for nitrates [12]. The control group included 20 apparently healthy individuals, and the NOx content in their blood serum was 25–58 μmol/L.
Method for determining endothelium-dependent vasodilation of the brachial artery in reactive hyperemia test was used to evaluate the endothelial function [13]. The method is based on determining the growth of the diameter of the brachial artery (dBA) in response to mechanical stimulation (transient occlusion of the shoulder as a result of compression of the sphygmomanometer cuff above the location of the vessel). In normal circumstances, post-occlusive blood flow is characterized by a peak increase in volume and linear velocity that occurs in the first 30 seconds after the removal of occlusion, with a gradual decrease in speed. In response to an increase in blood flow, there is a temporary increase in the shear stress on the endothelium, which, in turn, is accompanied by the release of substances that have vasodilational activity, which causes an increase in dBA. Toshiba Xario ultrasound machine with a 7.5 MHz multifrequency linear sensor was used to assess the changes in dBA (Fig. 1).
Endothelial function index (EFI) (response to the blood flow increase) was calculated as the difference between dBA after decompression and baseline, expressed as a percentage:
An increase in dBA by more than 20 % indicated a normal endothelial function (NEF), by 10–20 % — a decreased endothelial function (DEF), by less than 10 % — endothelial dysfunction (EDF).
The control group included 20 healthy individuals of representative age and sex.
Descriptive statistics was used for statistical analysis of the data; the comparison of the mean values of variables was carried out using parametric methods (Student’s t-test) for the normal distribution of the data expressed in the interval scale.
The correspondence of the characteristics distribution to the normal distribution law was verified using the Shapiro-Wilk test. In other cases, a non-parametric method was applied (Mann-Whitney U-test).
To compare the particle distribution of two or more variables, the χ2 test was used. Correlation analysis was performed by Pearson (for data expressed in the interval scale) and Spearmen methods (for data not expressed in the interval scale).
All calculations were performed in SPSS 9.0 for Windows [14].
Results and discussion
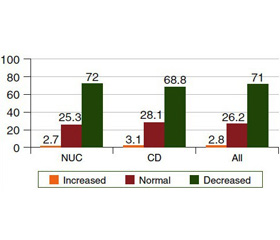
The analysis showed a significant decrease of NOx content in patients with NUC. The mean NOx values were significantly different from the control group and were reduced: in the main group of patients — 1.7-fold ((23.83 ± 1.15) μmol/L versus (41.65 ± 5.55) μmol/L, p < 0.01), in NUC patients — also 1.7-fold ((24.74 ± 1.47) μmol/L versus (41.65 ± 5.55) μmol/ L, p < 0.01), and in CD patients — 1.9-fold ((21.70 ± 1.70) μmol/L versus (41.65 ± 5.55) μmol/L, p < 0.001). An intergroup analysis showed that in NUC and CD groups, the vast majority of patients had a lower NOx content: 72.0 (p < 0.001) and 68.8 % (p < 0.001), respectively, as compared to controls (Fig. 2).
/42-2.jpg)
The content of NOx in the blood serum of patients with different nutritional status varied as follows: 1.8-fold decreased in group І ((23.79 ± 1.62) μmol/L versus (41.65 ± 5.55) μmol/L, p < 0.01), 1.9-fold decreased in group ІІ ((22.12 ± 2.32) μmol/L versus (41.65 ± 5.55) μmol/L, p < 0.01), and 1.7-fold decreased in group ІІІ ((25.12 ± 2.26) μmol/L versus (41.65 ± 5.55) μmol/L, p < 0.01). Thus, a significant reduction of serum NOx levels in chronic IBD patients is shown regardless of nutritional status. Such a decrease in the synthesis of NO occurs more often with prolonged and severe influence of adverse factors and corresponds to the stage of exhaustion. This may lead to further decrease in protective functions of the vascular endothelium.
Taking into account the detected decrease in serum NOx content, it was decided to investigate the state of the vascular endothelium in chronic IBD patients.
Results of endothelium-dependent vasodilation of the brachial artery by reactive hyperemia test in the examined patients are presented in Table 1.
According to the presented data, changes of vascular endothelium were detected in 76.7 % of patients. Patients with DEF prevailed in the structure of changes (49.2 %), patients with EDF were present twice less frequently (27.5 %). The mean values of the dBA increase rate were lower than normal values and corresponded to DEF (Table 2, Fig. 3).
Analysis of nosologies showed that changes in vascular endothelium were detected in 62 (76.5 %) patients with NUC and in 31 (79.4 %) CD patients, mainly due to decreased endothelial function (Fig. 4). There was a positive correlation between the percentage of dBA increase and the age of patients (r = 0.22, p = 0.015), duration of the disease (r = 0.21, p = 0.22). In the group of CD patients, an additional correlation between the percentage of dBA increase and the erythrocyte sedimentation rate has been found (r = 0.35, p = 0.03) (data are not given).
In NUC patients, DEF was detected in 43.2 % of cases, EDF — in 33.3 %, and in CD patients — in 64.1 and 15.4 % of cases, respectively. The statistically significant differences between nosological groups were not found.
We further investigated the function of vascular endothelium depending on patients’ nutritional status. The results of endothelium-dependent vasodilation of the brachial artery determined by the reactive hyperemia test showed that the percentage of dBA increase was smaller both in group I and group II patients compared to controls (Table 3).
Group III patients were characterized by the lowest ave–rage percentages of dBA increase. In addition, in group II patients, dBA increase was also lower than in the control group. A more detailed analysis revealed changes in the vascular endothelium in 53 (75.7 %), 15 (75.0 %) and 25 (83.4 %) patients of group I, II and III, respectively, mainly due to decreased endothelial function.
Thus, a study of the functional status of the vascular endothelium by the reactive hyperemia test with ultrasound revealed disorders in 76.7 % of chronic IBD patients, with a predominance of DEF in 50.0 % and EDF in 26.7 % of cases. More significant changes, both in the incidence of violations and in the percentage of dBA increase, were found in NUC patients as compared to CD patients. In patients with nutritional deficiency, changes in the vascular endothelium were observed in 75.4 % of cases, while the endothelium-dependent vasodilation of the brachial artery was significantly hig–her when compared to the patients with normal nutritional status — (17.21 ± 0.76) mm vs. (14.45 ± 0.45) mm, respectively.
Conclusions
1. It has been shown that 71 % of chronic IBD patients (72 % of individuals with NUC and 68.8 % of CD patients) demonstrated statistically significant decrease in serum NOx content, which may cause the violation of the protective functions of the vascular endothelium, which in turn confirms inadequate activation of protective antioxidant system and leads to the disease exacerbation and its chronic course. The probable decrease in serum NOx content in chronic IBD patients did not depend on their nutritional status.
2. Dysfunction of the vascular endothelium was detected in 76.7 % of the examined patients, with predominance of DEF (in 50.0 % of them). Patients with NUC had more pronounced changes in the incidence of identified violations and percentage of dBA increase as compared to those with CD. Changes in the vascular endothelium were observed in 75.4 % of the reduced nutritional status cases, while the indexes of endothelium-dependent vasodilation of the brachial artery were significantly higher compared to patients with normal nutritional status (p < 0.05).
Conflicts of interests. Authors declare the absence of any conflicts of interests that might be construed to influence the results or interpretation of their manuscript.
Список литературы
1. Alexakis C. Systematic review with meta-analysis: the impact of a depressive state on disease course in adult inflammatory bowel disease / C. Alexakis, S. Kumar, S. Saxena, R. Pollok // Aliment. Pharmacol. Ther. — 2017. — Vol. 46 (3). — P. 225-235. doi: 10.1111/apt.14171.
2. Степанов Ю.М. Застосування препаратів 5-аміносаліцилової кислоти в лікуванні запальних захворювань кишечника / Ю.М. Степанов, М.В. Стойкевич, О.В. Сорочан // Гастроентерологія. — 2016. — № 3 (51). — С. 80-87.
3. Степанов Ю.М. Хронічні запальні захворювання кишечника: особливості епідеміології в Україні / Ю.М. Степанов, І.Ю. Скирда, О.П. Петішко // Гастроентерологія. — 2017. — № 2 (51). — С. 11-19.
4. Русин В.І. Динаміка показників дисфункції ендотелію у хворих на хронічний панкреатит після холецистектомії під впливом L-аргініну L-глутамату / В.І. Русин, Є.С. Сірчак, Н.Ю. Курчак, О.М. Москаль // Здобутки клінічної і експериментальної медицини. — 2014. — № 1. — C. 101-103.
5. Калинкина Н.В. Особенности метаболизма оксида азота под влиянием различных кумулятивных доз антрациклиновых препаратов: Автореф. дис… канд. мед. наук: 14.01.11 / Н.В. Калинкина. — Донецк, 2010. — 6 с.
6. Никитина В.В. Влияние концентраций оксида азота и активности оксистата на развитие воспалительных изменений сосудистой стенки / В.В. Никитина, Н.Б. Захарова, Г.П. Гладилин, Г.В. Коршунов // Клиническая лабораторная диа–гностика. — 2014. — № 5. — С. 11-13.
7. Storch A.S. Methods of Endothelial Function Assessment: Description and Applications / A.S. Storch, J.D. Mattos, R. Alves [et al.] // International Journal of Cardiovascular Sciences. — 2017. — Vol. 30 (3). — P. 262-27. doi: 10.5935/2359-4802.20170034.
8. Vizzardi E. Noninvasive assessment of endothelial function: the classic methods and the new peripheral arterial tonometry / E. Vizzardi, M. Gavazzoni, P. Della Pina [et al.] // J. Investig. Med. — 2014. — Vol. 62(6). — P. 856-64. doi: 10.1097/JIM.0000000000000096.
9. Бойко Т.И. Состояние функции сосудистого эндотелия у больных с хроническими воспалительными заболеваниями кишечника / Т.И. Бойко, М.В. Стойкевич, Е.В. Колбасина, Е.В. Сорочан // Сучасна гастроентерологія. — 2010. — № 1 (51). — С. 5-10.
10. Flammer A.J. Three decades of endothelium research: from the detection of nitric oxide to the everyday implementation of endothelial function measurements in cardiovascular diseases / A.J. Flammer, T.F. Lüscher // Swiss Med. Wkly. — 2010. — 140:w13122. doi: 10.4414/smw.2010.13122.
11. Шабров А.В. Современные методы оценки эндотелиальной дисфункции и возможности их применения в практической медицине / А.В. Шабров, А.Г. Апресян, А.Л. Добкес [и др.] // Рациональная фармакотерапия в кардиологии. — 2016. — 12 (6). — С. 733-742.
12. Метельская В.А. Скрининг-метод определения уровня метаболитов оксида азота в сыворотке крови / В.А. Метельская, Н.Г. Гуманова // Лабораторная диагностика. — 2005. — № 6. — С. 15-18.
13. Лебедев П.А. Диагностика функции сосудистого эндотелия у больных с сердечно-сосудистыми заболеваниями / П.А. Лебедев, Л.И. Калакутский, С.П. Власова, А.П. Горлов: Метод. указания. — Самара, 2004. — 18 с.
14. Енюков И.С. Методы, алгоритмы, программы многомерного статистического анализа / И.С. Енюков. — М.: Финансы и статистика, 1986. — 232 с.

/42-1.jpg)
/42-2.jpg)
/43-1.jpg)
/43-2.jpg)
/44-1.jpg)