
Журнал "Гастроэнтерология" Том 53, №4, 2019
Вернуться к номеру
Цитомегаловірусна і змішані вірусні інфекції в пацієнтів iз запальними захворюваннями кишечника
Авторы: G.H. Babayeva
Azerbaijan State Advanced Training Institute for Doctors named after A. Aliev, Baku, Azerbaijan
Рубрики: Гастроэнтерология
Разделы: Клинические исследования
Версия для печати
Актуальність. Питання поширеності опортуністичних інфекцій в осіб iз запальними захворюваннями кишечника (ЗЗК) залишається актуальним. Особливу увагу серед опортуністичних інфекцій приділяється цитомегаловірусній (ЦМВ) інфекції. Клінічна активність ЦМВ-асоційованого ЗЗК, його тривалість і ступінь тяжкості, а також використання стероїдів і анти-ФНП-α-агентів були ідентифіковані як фактори ризику несприятливих наслідків. У діагностиці ЦМВ важливо не просто виявити наявність вірусу в організмі пацієнта, але й уточнити його етіологічну роль у розвитку захворювання. У цей час рекомендується проведення скринінгу на ЦМВ у всіх пацієнтів iз ЗЗК при гормональній резистентності, втрати ефекту від підтримуючої терапії та при тяжких епізодах захворювання. Мета дослідження: оцінка частоти виявлення ізольованої цитомегаловірусної інфекції і змішаних (герпес та парвовірус В19) вірусних інфекцій у пацієнтів iз ЗЗК та їх вплив на активність захворювання. Матеріали та методи. Обстежено 189 осіб iз ЗЗК, 102 з виразковим колітом і 87 з хворобою Крона, серед них 98 жінок та 91 чоловік. Вік пацієнтів становив від 16 до 63 років, у середньому (41,4 ± 4,8) року. Крім стандартного клініко-ендоскопічного обстеження відповідно до положень Європейської організації з вивчення хвороби Крона і виразкового коліту (ЕССО), активність захворювання оцінювалася за показниками високочутливого С-реактивного білка, гомоцистеїну, вітаміну D у сироватці крові, альбуміну в сечі, кальпротектину і лактоферину в калі. Усім пацієнтам проведено серологічне дослідження крові методом імуноферментного аналізу на специфічні антитіла до герпесвірусів і IgG-/IgM-антитіла до парвовірусу В19, а також визначення ДНК вірусів простого герпесу 1, 2, 6-го типів, вірусу Епштейна — Барр, цитомегаловірусу, герпесу зостер методом полімеразної ланцюгової реакції. В усіх пацієнтів також визначали рівні цитокінів у крові (фактор некрозу пухлини α, інтерлейкіни 1β, -2, -4, -6, -8, -10, -18). Результати. У пацієнтів iз ЗЗК частота виявлення ізольованої цитомегаловірусної інфекції становить, за нашими даними, 19,5 %, а з урахуванням змішаних уражень — 29,6 %. Клініко-ендоскопічна картина (рефрактерність до базисної терапії, невідповідність між ендоскопічною картиною і патоморфологічним висновком), а також дані лабораторних досліджень вказують на більш тяжкий перебіг захворювання за наявності цитомегаловірусної інфекції. Висновки. Отримані дані дозволяють нам рекомендувати на додаток до протоколiв ЕССО визначення наявності опортуністичних інфекцій у пацієнтів iз вперше виявленим ЗЗК до початку базисної терапії, не чекаючи на розвиток рефрактерних до лiкування форм захворювання.
Актуальность. Вопрос распространенности оппортунистических инфекций у лиц с воспалительными заболеваниями кишечника (ВЗК) остается актуальным. Особое внимание среди оппортунистических инфекций уделяется цитомегаловирусной (ЦМВ) инфекции. Клиническая активность ЦМВ-ассоциированного ВЗК, его длительность и степень тяжести, а также использование стероидов и анти-ФНО-α-агентов были идентифицированы как факторы риска неблагоприятных исходов. В диагностике ЦМВ важно не просто выявить наличие вируса в организме пациента, но и уточнить его этиологическую роль в развитии заболевания. В настоящее время рекомендуется проведение скрининга на ЦМВ у всех пациентов с ВЗК при гормональной резистентности, потере эффекта от поддерживающей терапии и при тяжелых эпизодах заболевания. Цель исследования: оценка частоты выявления изолированной цитомегаловирусной инфекции и смешанных (герпес и парвовирус В19) вирусных инфекций у пациентов с ВЗК и их влияние на активность заболевания. Материалы и методы. Обследовано 189 пациентов с ВЗК, 102 с язвенным колитом и 87 с болезнью Крона, среди них 98 женщин и 91 мужчина. Возраст пациентов составлял от 16 до 63 лет, в среднем (41,4 ± 4,8) года. Кроме стандартного клинико-эндоскопического обследования в соответствии с положениями Европейской организации по изучению болезни Крона и язвенного колита (ЕССО), активность заболевания оценивалась по показателям высокочувствительного С-реактивного белка, гомоцистеина, витамина D в сыворотке крови, альбумина в моче, кальпротектина и лактоферрина в кале. Всем пациентам проведено серологическое исследование крови методом иммуноферментного анализа на специфические антитела к герпесвирусам и IgG-/IgM-антитела к парвовирусу В19, а также определение ДНК вирусов простого герпеса 1, 2, 6-го типов, вируса Эпштейна — Барр, цитомегаловируса, герпеса зостер методом полимеразной цепной реакции. У всех пациентов также определяли уровни цитокинов в крови (фактор некроза опухоли α, интерлейкины 1β, -2, -4, -6, -8, -10, -18). Результаты. У пациентов с ВЗК частота выявления изолированной цитомегаловирусной инфекции составляет, по нашим данным, 19,5 %, а с учетом смешанных поражений — 29,6 %. Клинико-эндоскопическая картина (рефрактерность к базисной терапии, несоответствие между эндоскопической картиной и патоморфологическим заключением), а также данные лабораторных исследований указывают на более тяжелое течение заболевания при наличии цитомегаловирусной инфекции. Выводы. Полученные данные позволяют нам рекомендовать в дополнение к протоколам ЕССО определение наличия оппортунистических инфекций у пациентов с впервые выявленным ВЗК до начала базисной терапии, не дожидаясь развития рефрактерных к лечению форм заболевания.
Background. The issue of the prevalence of opportunistic infections in persons with inflammatory bowel disease (IBD) remains relevant. Among opportunistic infections, in particular, we would like to note Herpesviridae family (herpes simplex virus type 1 and 2), human herpesvirus type 3 (varicella zoster virus), human herpesvirus type 4 (Epstein-Barr virus), cytomegalovirus (CMV), or human herpesvirus type 5, human herpesvirus type 6 and parvovirus B19. Clinically marked herpes and parvovirus infections are frequent causes of systemic inflammation of the gastrointestinal tract. This is a serious problem, especially for persons with long-term immunosuppression, who have IBD, and special attention in this aspect is paid to cytomegalovirus infection. Clinical activity of CMV-associated IBD, its duration and severity, as well as the use of steroids and anti-TNF-α agents were identified as risk factors for adverse outcomes. It is important not only to detect the presence of viruses in the patient’s body, but also to clarify their etiological role in the development of the disease. According to the current European Crohn’s and Colitis Organisation (ECCO) protocols, all patients with IBD are recommended to be screened in hormone resistance, loss of effect from maintenance therapy and severe attacks of the disease. The addition of active CMV infection to IBD may likely be one of the causes of resistance to hormone and immunosuppressive therapy, as well as biological drugs, but this issue requires further researches. The purpose was to evaluate the frequency of detecting isolated cytomegalovirus infection and mixed (herpes and parvovirus B19) viral infections in patients with IBD and their influence on the disease activity. Materials and methods. One hundred and eighty-nine patients (98 women and 91 men) with IBD (102 with ulcerative colitis (UC) and 87 with Crohn’s disease (CD)) were examined. The age of patients was from 16 to 63 years (mean age (41.4 ± 4.8) years). In addition to standard clinical endoscopic examinations according to ECCO guidelines, disease activity was assessed by indicators of highly sensitive C-reactive protein, homocysteine, vitamin D in blood serum, albumin in urine, calprotectin and lactoferrin in feces. All patients underwent serological blood test by enzyme-linked immunosorbent assay for specific antibodies to herpesviruses and IgG/IgM antibodies to parvovirus B19, determination of DNA of herpes simplex viruses types 1, 2, 6, Epstein-Barr virus, cytomegalovirus, herpes zoster by a polymerase chain reaction in blood and tissues. All patients underwent determination of blood cytokines (tumor necrosis factor α, interleukins 1β, -2, -4, -6, -8, -10, -18). Results. Viral (herpes and parvovirus B19) infections in patients with IBD occurred in 81 cases (42.8 %): in 35 (40.2 %) of 87 patients with CD and in 46 (45.0 %) of 102 — with UC. Among patients with cytomegalovirus infection alone, 21 (11.1 % of the total number and 25.9 % of infected persons) suffered from UC and 16 (8.5 % of the total number and 19.7 % of infected persons) — from CD. In 26 (13.8 % of the total number and 32.1 % of infected persons) cases, mixed viral infections were detected — in 13 patients with CD and 13 with UC (6.9 % of the total number and 16.0 % of infected persons). In patients with IBD, the frequency of detecting isolated cytomegalovirus infection is 19.5 % of the total number and 45.6 % of infected persons; mixed viral infection was found in 13.8 % of the total number and 32.1 % of infected patients. The clinical endoscopic picture (resistance to basic therapy, the mismatch between the endoscopic picture and the pathomorphological conclusion), as well as laboratory data, indicate a more severe course of diseases in the presence of cytomegalovirus infection. Conclusion. The data obtained allow us to recommend, in addition to ECCO protocols, the determination of the presence of opportunistic (herpes and parvovirus B19) infections in patients with newly diagnosed IBD before starting basic therapy, without waiting for the development of disease forms refractory to therapy.
цитомегаловірусна інфекція; герпес і парвовiрус В19; змішані вірусні інфекції; запальні захворювання кишечника; виразковий коліт; хвороба Крона
цитомегаловирусная инфекция; герпес и парвовирус В19; смешанные вирусные инфекции; воспалительные заболевания кишечника; язвенный колит; болезнь Крона
cytomegalovirus infection; herpes and parvovirus B19; mixed viral infections; inflammatory bowel disease; ulcerative colitis; Crohn’s disease
Introduction
The prevalence of opportunistic infections in individuals with inflammatory bowel disease (IBD) remains relevant. Clinically expressed herpes and parvovirus infections are a common causes of systemic inflammation of the gastrointestinal tract. This is a serious problem, especially for people with long-term immunosuppression. Particular attention among opportunistic infections is paid to cytomegalovirus infection (CMV). The clinical activity of CMV-associated IBD, the duration and severity of the disease, and the use of steroids and anti-TNF-α agents have been identified as risk factors for adverse outcomes. In the diagnosis of CMV, it is important not only to detect the presence of the virus in the patient’s body, but also to clarify its etiological role in the development of the disease. The most significant here are virological and serological methods. Currently, screening for CMV is recommended for all patients with IBD in hormone resistance, loss of effect from ongoing maintenance therapy and in severe attacks of the disease. The addition of active CMV infection to IBD may likely be one of the causes of resistance to hormone and immunosuppressive therapy, as well as biological drugs, however, this issue requires further researches.
Why is it so important to determine the presence of cytomegalovirus infection in patients with IBD?
Human CMV (Cytomegalovirus hominis) is an anthroponotic viral disease, belongs to the family Herpesviridae (has the specific name human herpesvirus (HHV) type 5). CMV is characterized by polyhistiotropy, which might lead to a variety of clinical forms of the disease involving various organs and systems of the body in the pathological process. This circumstance gives the problem of CMV an interdisciplinary nature [1]. Three virus strains were registered: AD 169, Davis, and Kerr. The viral envelope consists of proteins, which also participate in the formation of the immune response: glycoproteins H and B [1, 2].
In acute CMV, the virus infects epithelial cells, including enterocytes and colonocytes, with the formation of giant cells with intranuclear inclusions of cytomegaloviruses in the tissues and organs. Cytomegaloviruses, which are lymphohistiocytic infiltrates, cause productive vasculitis with damage to all layers of the vessel wall and the outcome in sclerosis. This vascular lesion serves as the basis for thrombosis that leads to ischemic damage to organs and tissues, which is the basis of pathogenesis [1, 3].
CMV can suppress cellular immunity due to virus replication in the cells of the immune system, as well as the ability to slow replication, relatively low pathogenicity and lifelong persistence in humans with periodic reactivation [1, 3, 4]. There may be periods of reactivation of the infection with the secretion of the virus from the nasopharynx and in the urogenital tract.
Infection is often asymptomatic. In 5 % of patients, it can occur in the form of mononucleosis-like syndrome with high fever, myalgia, arthralgia, polylymphadenopathy, hepa–tosplenomegaly. The lesion is often generalized [3]. A wide range of organ lesions, including gastrointestinal tract organs, is associated with CMV. The disease can cause ulcera–tive defects of the digestive tract: ulcerative necrotic lesions of the esophagus, colon, less often — of the small intestine and stomach [1, 5, 6]. In repeated infection or reactivation of CMV against the background of immunosuppression, active replication of the virus begins, a manifestation of the disease is possible with a tendency to the generalization of the process [5, 6].
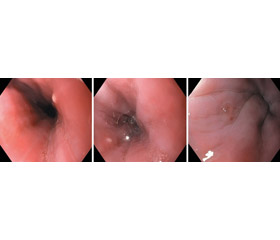
Typical clinical signs of CMV esophagitis are fever, difficulty swallowing, severe chest pain during passage of the food lump, and the absence of the effect of antifungal therapy. The endoscopic picture is characterized by the presence of shallow rounded ulcers or erosion in the distal esophagus (Fig. 1).
/62-1-1.jpg)
CMV has a tropism for actively proliferating tissues of the gastrointestinal tract, therefore, patients with IBD have an increased risk of CMV colitis [1–7]. The clinical picture of CMV colitis or enterocolitis includes severe abdominal pain, diarrhea, weakness, severe weight loss; blood in the stool is also possible.
For the endoscopic picture, the detection of erosion on the mucous membrane of the colon and, less commonly, the small intestine is pathognomonic; the presence of typical endoscopic features, including longitudinal ulcers, mucosal lesions with cobblestone appearance, discrete lesions, mucosal defects, perforated ulcer, creates difficulties in endoscopic verification of the diagnosis of ulcerative colitis (UC) and Crohn’s disease (CD) (Fig. 2).
/63-1-1.jpg)
IBD is characterized by relapses and periods of remission. However, clinical signs such as abdominal pain, diarrhea, and rectal bleeding are not specific to ulcerative colitis and Crohn’s disease. Therefore, the differential diag–nosis should include a wide range of inflammatory or infectious diseases that mimic IBD, and can also complicate the course of the disease. Superinfection of CMV or Clostridium difficile can aggravate intestinal inflammation, especially in immunocompromised individuals. CMV in patients with ulcerative colitis is associated with a severe course of the disease and hormonal dependence, it is necessary to accurately determine the cause, which aggravates the course of IBD [7].
Y. Li et al. conducted a 5-year retrospective study in IBD patients, the result of which was a conclusion that in mixed infection (CMV and C.difficile), worse outcomes are observed in patients with UC and CD [8]. Cytomegalovirus disease in patients with IBD is often a result of viral reactivation against the background of ongoing immunosuppression [9–13]. C. Rowan et al. (2018) recommend diagnostic tests to be carried out for the detection of CMV markers in all patients with IBD occurring with febrile condition [9]. Research by T.M. Nowacki et al. also confirms the pathogenic significance of CMV in ulcerative colitis, where the relationship of exacerbation of ulcerative colitis with reactivation of CMV was proved, especially in patients with wea–kened immunity [10, 11].
CMV etiology of the disease is common in patients with severe IBD. The clinical activity of CMV-associated IBD, the duration and severity of the disease, especially when –using steroids and anti-TNF-α agents, were identified as risk factors for severe outcomes (p < 0.05 each) [10–14].
The multifaceted nature of CMV does not allow one to diagnose an infection clinically; therefore, the decisive role belongs to specific laboratory diagnosis, which is based on various methods for detecting the causative agent: identification of viral DNA, its antigens, specific antibodies, morphological picture [1, 14, 15]. In the diagnosis of CMV, it is important to establish not only the presence of the virus in the patient’s body, but also its etiological role in the development of this disease. The most significant in our time are virological (isolation of CMV, detection of its antigens) and serological methods (determination of specific IgM and IgG antibodies by enzyme-linked immunosorbent assay (ELISA), avidity of anti-CMV IgG). IgG avidity index of anti-CMV above 50–60 % indicates the presence of highly avid antibodies in the serum — markers of a past infection or persistent infection and elimination of the primary CMV infection in the last 3–4 months. Highly avid IgG antibodies persist for life. CMV reactivation is judged by the appearance of anti-CMV IgM. It is very important to take into account that the level of specific antibodies and their titer are not indicators determining the degree of infection activity, since they depend on individual immune reactivity.
In the last decade, the leading place in the diagnosis of CMV belongs to the molecular genetic method for determining CMV DNA — polymerase chain reaction (PCR). PCR is used to detect and quantify CMV DNA in various biological fluids and tissues. Thus, according to the findings of Y. Tsuchido et al. (2018), the use of PCR for biopsies showed good diagnostic indicators when detecting CMV in patients [11]. The combination of virological and serological methods is optimal for the diagnosis of CMV and determines the degree of its activity. The etiological role of the virus in CMV-associated somatic disease is determined based on the correlation of the results of laboratory and clinical research methods [11].
IBD is treated with drugs that suppress the immune system, which increases the risk of developing infectious complications [12, 16]. Against the background of such therapy, reactivation of latent viral infections, including CMV, often occurs. It is believed that the association with CMV may be one of the causes of the severe course of IBD and hormone resistance, as well as resistance to other ongoing therapy, including anti-TNF-α drugs [13, 16, 17]. For patients with IBD and clinically expressed CMV infection, specific antiviral therapy is extremely important. Before specific treatment begins, immunosuppressive therapy should be discontinued. Control using ELISA or PCR is carried out at the end of the main course of therapy. Immunosuppressive therapy can be resumed after receiving negative results of tissue PCR [1, 12, 16].
Nucleotide analogues (ganciclovir, valganciclovir) are used as antiviral chemotherapy drugs for the treatment of CMV infection. They are effective inhibitors of viral DNA replication [1, 5, 13, 16, 17]. The antiviral effect of ganciclovir is associated with the formation of ganciclovir triphosphate and competitive inhibition of DNA polymerase, as well as direct incorporation into viral DNA, which inhi–bits virus replication. The drug is stored in the cytoplasm of virus-infected cells for several days [1, 13, 14, 17, 18].
The standard course of therapy is the use of ganciclovir at a dose of 5 mg/kg twice a day or valganciclovir 900 mg twice a day for 14–21 days until the symptoms of the disease disappear and DNA virus is eliminated from the patient’s blood. In order to prevent the recurrence of the disease in patients in a state of immunosuppression, a maintenance course of valganciclovir 900 mg twice a day for a month is carried out [17–19]. The use of interferons and interferon inducers (for example, cycloferon, viferon) in combination with antiviral drugs also leads to positive results [4, 13, 14, 17, 18].
The purpose: to assess the frequency of detecting isolated cytomegalovirus infection and mixed viral (herpes and parvovirus B19) infection in patients with IBD and its effect on disease activity.
Materials and methods
One hundred and eighty-nine patients (98 women and 91 men) with IBD (102 with ulcerative colitis and 87 with Crohn’s disease) were examined. The age of patients was from 16 to 63 (mean of (41.4 ± 4.8)) years. In addition to standard clinical endoscopic examinations according to European Crohn’s and Colitis Organisation (ECCO) guidelines, disease activity was assessed by indicators of highly sensitive C-reactive protein (CRP), homocysteine, vitamin D in blood serum, albumin in urine, calprotectin and lactoferrin in feces. All patients underwent a serological blood test by ELISA for specific antibodies to herpesviruses and IgG/IgM antibodies to parvovirus B19, the determination of DNA to herpes simplex virus types 1, 2, 6, Epstein-Barr virus (EBV), cytomegalovirus, herpes zoster by PCR in blood and tissues. All patients underwent determination of blood cytokines (tumor necrosis factor-α (TNF-α), interleukins (IL) 1β, -2, -4, -6, -8, -10, -18).
Chronic active EBV infection was diagnosed based on the detection of antinuclear antibodies to EBV (EBV-NA1 IgG) in excess of the permissible indicators by 4 or more times, as well as the presence of EBV-VCA IgM, EBV-EA IgG and determination of EBV DNA in blood cells and/or biopsy samples of the intestinal mucosa in a concentration from 1,000 copies/ml.
Chronic active CMV was established based on the detection of specific IgG antibodies in a titer of at least 1 : 3,200 (i.e., 4 times higher than the permissible norm), IgM and detection of CMV DNA in blood cells and/or biopsy samples of the intestinal mucosa in a concentration from 1,000 copies/ml.
Chronic active infection of herpes simplex virus (HSV) types 1 and 2 was diagnosed based on the detection of specific IgG antibodies in a titer of at least 1 : 3,200 (i.e., 4 times exceeded the permissible norm), IgM antibodies and detection of HSV 1–2 DNA in blood cells and/or biopsy specimens of the intestinal mucosa in a concentration of 1,000 copies/ml.
Active human herpesvirus type 6 infection was established based on the detection of DNA of this virus in blood cells and/or biopsy specimens of the intestinal mucosa in a concentration of 1,000 copies/ml.
Results and discussion
The results are presented in Fig. 3, 4 and Table 1.
/64-1-1.jpg)
/65-1-1.jpg)
As can be seen from Table 1, viral infections in patients with IBD occurred in 81 cases (42.8 %): in 35 (40.2 %) of 87 patients with CD and in 46 (45.0 %) of 102 — with UC (Fig. 3).
At the same time, in 55 patients (29.1 % of the total number and 67.9 % of infected persons), isolated viral infection was detected: Epstein-Barr virus — in 2 (1.1 % of the total number and 2.4 % of infected persons), cytomegalovirus — in 37 (19.5 % of the total number and 45.6 % of infected persons), and parvovirus — in 16 (8.4 % of the total number and 19.7 % of infected persons). Among patients with isolated cytomegalovirus infection, 21 (11.1 % of the total number and 25.9 % of infected persons) suffered from UC and 16 (8.5 % of the total number and 19.7 % of infected persons) — from CD.
In 26 cases (13.8 % of the total number and 32.1 % of infected persons), mixed viral infections were detected — in 13 patients with CD and 13 with UC (6.9 % of the total number and 16.0 % of infected persons).
The following combinations of mixed viral infections were noted: CMV + HSV 1–2 — in 5 cases (2 — UC and 3 — CD), CMV + EBV — in 11 (5 — UC and 6 — CD), EBV + HHV-6 — in 2 (UC), EBV + parvovirus B19 — in 5 (3 — UC and 2 — CD), EBV + parvovirus B19 + CMV — in 3 (1 — UC and 2 — CD).
As a result, cytomegalovirus infection was detected in 56 patients (29.6 % of the total number and 69.1 % of infected persons): in 37 cases — alone (19.5 % of the total number and 45.6 % of infected persons) and in 19 — in the form of mixed viral infections (10 % of the total number and 23.4 % of infected persons).
Clinical endoscopic and laboratory indicators of inflammatory activity in IBD were significantly higher in patients with viral infections (p < 0.05). Thus, the values of CRP, platelets, lactoferrin and calprotectin were significantly higher in patients with concomitant viral damage (p < 0.05). This pattern was observed both in UC and CD. Moreover, the markers of inflammation were greatest in the presence of cytomegalovirus infection, although this difference did not reach the threshold of statistical significance.
ECCO recommends screening for CMV infection in all patients with IBD in hormone resistance, loss of effect from ongoing maintenance therapy and severe attacks of the disease [16]. Based on clinical studies in China and other countries, the Gastroenterological Society of the Chinese Medical Association published a consensus opinion in 2018 that patients with IBD are at high risk of opportunistic infections [19].
The following provisions were formulated:
1. Screening for CMV is recommended for patients with acute severe ulcerative colitis with resistance to glucocorticoids.
2. The detection of specific anti-CMV IgM antibo–dies and/or pp65 CMV (≥ 1 CMV-positive cells in every 150,000 leukocytes) and/or CMV DNA in the blood of –real-time quantitative PCR (qPCR) suggests an active form of CMV.
3. The gold standard for the diagnosis of CMV colitis is a positive pathomorphological study on H- and E-staining in combination with positive immunohistochemistry and/or positive qPCR for CMV DNA in the tissues of the colon mucosa.
4. Antiviral therapy is recommended for CMV DNA > 1,200 copies/ml blood (qPCR).
5. Typical endoscopic features, including mucosal defect, perforated ulcer, longitudinal ulcers, such as cobblestone appearance, and discrete lesions, suggest CMV colitis. This requires a routine biopsy with differential diagnosis.
6. Antiviral therapy should be started timely in patients with severe steroid-resistant IBD associated with CMV. The decision to stop taking or reduce the dose of immunosuppressants should be considered based on the assessment of all the pros and cons.
7. A three- to six-week course of antiviral therapy is re–commended for patients with IBD associated with CMV.
Conclusions
Viral infections in patients with IBD occurred in 81 ca–ses (42.8 %): in 35 (40.2 %) of 87 patients with CD and in 46 (45.0 %) of 102 with UC.
Among patients with isolated cytomegalovirus infection, 21 (11.1 % of the total number and 25.9 % of infected persons) suffered from UC and 16 (8.5 % of the total number and 19.7 % of infected persons) — from CD. In 26 (13.8 % of the total number and 32.1 % of infected persons) cases, mixed viral infections were detected — in 13 patients with CD and 13 with UC (6.9 % of the total number and 16.0 % of infected persons). In patients with IBD, the frequency of detecting isolated cytomegalovirus infection is 19.5 % of the total number and 45.6 % of infected persons; mixed viral infection was detected in 13.8 % of the total number and 32.1 % of the number of infected patients.
The clinical endoscopic picture (resistance to basic the–rapy, the mismatch between the endoscopic picture and the pathomorphological conclusion), as well as laboratory data indicate a more severe course of diseases in the presence of cytomegalovirus infection.
The data obtained allow us to recommend, in addition to ECCO protocols, the determination of the presence of opportunistic (herpes and parvovirus B19) infections in patients with newly diagnosed IBD before starting basic the–rapy, without waiting for the development of disease forms refractory to therapy.
Conflicts of interests. Author declares the absence of any conflicts of interests and their own financial interest that might be construed to influence the results or interpretation of their manuscript.
- Khalif IL, Alexandrov TL, Kisteneva LB. Cytomegalovirus infection in inflammatory bowel diseases. Koloproktologiв. 2019;18(67):119-126. doi: 10.33878/2073-7556-2019-18-1-119-126. (in Russian).
- Knyazev OV, Parfenov AI, Kagramanova AV, et al. Long-term infliximab therapy for ulcerative colitis in real clinical practice. Terapevticheskiy arkhiv. 2016;88(8):6-52. (in Russian).
- Zhukova LI, Lebedev VV, Gorodin VN, Zotov SV, Kovalevskaya OI, Chakhoyan PO. Acute cytomegalovirus infection in adult HIV-negative patients. Infectious Diseases. 2013;11(1):37-43. (in Russian).
- Kochkina SS, Sitnikova EP. Specific features of cytomegalovirus infection: literature review. Doctor. Ru. 2016;(123):62-67. (in Russian).
- Tserah TM, Polynskaya AV. Cytomegalovirus associated with immunosuppression. Voennaia meditsina. 2016;2(39):145-146. (in Russian).
- Shestakova IV, editor. Tsitomegalovirusnaia infektsiia u vzroslykh (iskliuchaia bol'nykh VICh-infektsiei): klinicheskie rekomendatsii [Cytomegalovirus in adults (excluding patients with HIV infection): clinical guidelines]. Moscow; 2014. 74 p. (in Russian).
- Gecse KB, Vermeire S. Differential diagnosis of inflammatory bowel disease: imitations and complications. Lancet Gastroenterol Hepatol. 2018 Sep;3(9):644-653. doi: 10.1016/S2468-1253(18)30159-6.
- Li Y, Xu H, Xu T, et al. Case-Control Study of Inflammatory Bowel Disease Patients with and without Clostridium difficile Infection and Poor Outcomes in Patients Coinfected with C. difficile and Cytomegalovirus. Dig Dis Sci. 2018 Nov;63(11):3074-3083. doi: 10.1007/s10620-018-5230-1.
- Rowan C, Judge C, Cannon MD, et al. Severe Symptomatic Primary CMV Infection in Inflammatory Bowel Disease Patients with Low Population Seroprevalence. Gastroenterol Res Pract. 2018 Jun 28;2018:1029401. doi: 10.1155/2018/1029401.
- Nowacki TM, Bettenworth D, Meister T, et al. Novel score predicts risk for cytomegalovirus infection in ulcerative colitis. J Clin Virol. 2018 Aug;105:103-108. doi: 10.1016/j.jcv.2018.06.002.
- Tsuchido Y, Nagao M, Matsuura M,et al. Real-time quantitative PCR analysis of endoscopic biopsies for diagnosing CMV gastrointestinal disease in non-HIV immunocompromised patients: a diagnostic accuracy study. Eur J Clin Microbiol Infect Dis. 2018 Dec;37(12):2389-2396. doi: 10.1007/s10096-018-3387-3.
- Ciccocioppo R, Racca F, Scudeller L, et al. Differential cellular localization of Epstein-Barr virus and human cytomegalovirus sin the colonic mucosa of patients with active or quiescent inflammatory bowel disease. Immunol Res. 2016 Feb;64(1):191-203. doi: 10.1007/s12026-015-8737-y.
- Fajfr M, Štěpánová V. Cytomegalovirus and its relationship to chronic inflammatory bowel diseases and tumors. Klin Mikrobiol Infekc Lek. 2013 Sep;19(3):103-6. (in Czech).
- Ford AC, Peyrin-Biroulet L. Opportunistic infections with anti-necrosis factor-α therapy in inflammatory bowel disease: meta-analysis of randomized controlled trials. Am J Gastroenterol. 2013 Aug;108(8):1268-76. doi: 10.1038/ajg.2013.138.
- Johnson J, Affolter K, Boynton K, Chen X, Valentine J, Peterson K. CMV Disease in IBD: Comparison of Diagnostic Tests and Correlation with Disease Outcome. Inflamm Bowel Dis. 2018 Jun 8;24(7):1539-1546. doi: 10.1093/ibd/izy045.
- Rahier JF, Magro F, Abreu C, et al. Second European evidence-based consensus on the prevention, diagnosis and management of opportunistic infections in inflammatory bowel di–sease. J Crohns Colitis. 2014 Jun;8(6):443-68. doi: 10.1016/j.crohns.2013.12.013.
- Markova DO, Nasyrov RA, Revanova MO. Cytomegalovirus infection in patients with inflammatory bowel disease. Pediatr. 2013;4(1):95-99. (in Russian).
- Galegov GA, Andronova VL. Chemotherapy for viral infections. In: L'vov DK, editor. Meditsinskaia virusologiia [Medical virsology]. Moscow: MIA; 2008. 87-92 pp. (in Russian).
- Inflammatory Bowel Disease Group, Chinese Society of Gastroenterology, Chinese Medical Association. Evidence-based consensus on opportunistic infections in inflammatory bowel disease (republication). Intest Res. 2018 Apr;16(2):178-193. doi: 10.5217/ir.2018.16.2.178.