
Международный эндокринологический журнал Том 15, №7, 2019
Вернуться к номеру
Стан йодного забезпечення дітей та жінок репродуктивного віку в західному регіоні України
Авторы: Pasyechko N.V., Chukur O.O., Krytskyy T.I., Bob A.O.
I. Horbachevsky Ternopil National Medical University, Ternopil, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
Актуальність. В Україні за останні роки спостерігається зростання частоти тиреоїдної патології. Абсолютна кількість випадків захворювання щитоподібної залози за останні 10 років зросла з 689 000 до 1 486 000, згідно з даними щодо поширення, що становить 941,6 і 4210,4 випадку на 100 000 населення відповідно. Частота патології щитоподібної залози (станом на 01.01.2018) становить 46 % від усіх ендокринологічних захворювань і посідає перше місце серед них. Основною причиною є незбалансованість мікроелементного і вітамінного складу в раціоні на тлі погіршення екологічної ситуації та техногенного забруднення довкілля. Метою дослідження було оцінити ступінь йодного дефіциту в населення західного регіону України та надати теоретичне обґрунтування подальшого подолання йододефіцитних станів. Матеріали та методи. Вивчення стану йодного забезпечення населення проводили серед вагітних жінок у першому триместрі вагітності (19–44 роки) та дітей шкільного віку (12–14 років), які проживають у західному регіоні України. Йодне забезпечення оцінювали з використанням неонатального скринінгу концентрації тиреотропного гормону в новонароджених, даних щодо частоти зоба за результатами пальпаторного обстеження, ультрасонографічного обстеження щитоподібної залози та медіани екскреції йоду з сечею. Результати. За даними неонатального скринінгу частота гіпертиреотропінемії становила в середньому 3,52 ± 0,30 % в популяції, що відповідає легкому ступеню йодної недостатності. За результатами ультрасонографічного обстеження щитоподібної залози частота виявлення зоба в дітей становить 38 %, а у вагітних жінок — 36 %, що є характерним для тяжкого ступеня йодного дефіциту. Результати визначення медіани йодурії в дітей показали недостатнє йодне забезпечення в 20 %, концентрація йоду в сечі в середньому становила 99,69 ± 35,42 мкг/л. У 30 % дітей спостерігалось надлишкове надходження йоду в організм, та 50 % обстежених дітей мали оптимальне забезпечення йодом. Нестачу йоду в раціоні вагітних було виявлено в 43,3 % обстежених (медіана йодурії 81,96 ± 42,53 мкг/л). У 26,7 % вагітних концентрація йоду в сечі відповідала нормальному інтервалу, надлишкове надходження йоду в організм при медіані понад 230 мкг/л було виявлене в 30 % вагітних. Висновки. Оцінка йодного забезпечення населення західного регіону України свідчить про тяжкий ступінь йодної недостатності, що вимагає термінового впровадження загальнонаціональної програми профілактики.
Актуальность. В Украине за последние годы наблюдается рост тиреоидной патологии. Абсолютное количество случаев заболеваний щитовидной железы за последние 10 лет возросло с 689 000 до 1 486 000, согласно данным относительно распространения, что составляет 941,6 и 4210,4 случая на 100 000 населения соответственно. Частота патологии щитовидной железы (по состоянию на 01.01.2018) составляет 46 % от всех эндокринологических заболеваний и занимает первое место среди них. Основной причиной является несбалансированность микроэлементного и витаминного состава в рационе на фоне ухудшения экологической ситуации и техногенного загрязнения окружающей среды. Целью исследования было оценить степень йодного дефицита у населения западного региона Украины и предоставить теоретическое обоснование дальнейшего преодоления йододефицитных состояний. Материалы и методы. Изучение состояния йодного обеспечения населения проводили среди беременных женщин в первом триместре беременности и детей школьного возраста, проживающих в западном регионе Украины. Йодное обеспечение оценивали с использованием неонатального скрининга концентрации тиреотропного гормона у новорожденных, данных относительно частоты зоба по результатам пальпаторного обследования, ультрасонографического обследования щитовидной железы и медианы экскреции йода с мочой. Результаты. По данным неонатального скрининга частота гипертиреотропинемии составляла в среднем 3,52 ± 0,30 % в популяции, что соответствует легкой степени йодной недостаточности. По результатам ультрасонографического обследования щитовидной железы частота выявления зоба у детей составляет 38 %, а у беременных женщин — 36 %, что характерно для тяжелой степени йодного дефицита. Результаты определения медианы йодурии у детей показали недостаточное йодное обеспечение у 20 %, концентрация йода в моче в среднем составляла 99,69 ± 35,42 мкг/л. У 30 % детей наблюдалось избыточное поступление йода в организм, и 50 % обследованных детей имели оптимальное обеспечение йодом. Недостаток йода в рационе беременных был выявлен у 43,3 % обследованных (медиана йодурии 81,96 ± 42,53 мкг/л). У 26,7 % беременных концентрация йода в моче отвечала нормальным интервалам, избыточное поступление йода в организм при медиане выше 230 мкг/л было обнаружено у 30 % беременных. Выводы. Оценка йодного обеспечения населения западного региона Украины свидетельствует о тяжелой степени йодной недостаточности, что требует немедленного внедрения общенациональной программы профилактики.
Background. In recent years, the incidence of thyroid gland pathology has increased in Ukraine. The absolute number of cases of thyroid diseases in Ukraine over the past 10 years has increased from 689,000 to 1,486,000, according to the prevalence rates, that is 941.6 and 4,210.4 cases per 100,000 of population, respectively. Thyroid pathology with its total frequency in the population (as of 01.01.2018) is 46 % of the total endocrinological morbidity and takes the first place among endocrinopathies. The main cause is imbalance of trace elements and vitamins in the diet against the environmental degradation and technogenic pollution. The purpose of the work was to evaluate the iodine deficiency degree in the population of the Western region of Ukraine. Materials and methods. The iodine supply in the population was assessed among the representative groups: the pregnant women (19–44 years) in the first trimester of pregnancy and the children of school age (12–14 years), residing in the Western region of Ukraine. Assessment of iodine supply was performed using epidemiological indicators: neonatal screening of thyroid-stimulating hormone concentration in newborns, goitre frequency found by palpation, ultrasonographic examination of the thyroid gland and the median of the urinary iodine excretion. Results. The frequency of hyperthyrotropinemia was 3.52 ± 0.30 %, which corresponds to a slight degree of iodine deficiency. The results of ultrasonographic examination revealed the goitre frequency in 38 % of children, and in 36 % of pregnant women, which corresponded to the severe degree of iodine deficiency in the region. The results of the median of ioduria in children showed an inadequate iodine content in 20 % of cases, and the urinary iodine concentration was on average 99.69 ± 35.42 μg/l. Lack of iodine in the diet of pregnant women was found in 43.3 % of the examined women (median of ioduria 81.96 ± 42.53 μg/l). The normal iodine concentration was found in 26.7 % of cases, excessed iodine intake with median of ioduria over 230 μg/l was registered in 30 % of women. Conclusions. The estimation of iodine maintenance in the population of the Western region of Ukraine demonstrated a severe degree of iodine deficiency that requires the urgent implementation of a nationwide prevention program.
йодний дефіцит; щитоподібна залоза; зоб; неонатальний скринінг; медіана йодурії; Україна
йодный дефицит; щитовидная железа; зоб; неонатальный скрининг; медиана йодурии; Украина
iodine deficiency; thyroid gland; goitre; neonatal screening; median of ioduria; Ukraine
Introduction
According to the World Health Organization (WHO), the pathological conditions associated with iodine deficiency take the third place in the list of the most common non-infectious diseases today [1]. WHO experts believe that one-third of the world population lives in areas with iodine deficiency in water and food and refers to the so-called risk group for the development of iodine deficiency disorders (IDD) [2]. Iodine deficiency (ID) is one of the most urgent health problems for more than 140 countries [3, 4]. Diseases prevention and elimination programs are carried out at the state level. The main coordinators of these programs are the relevant national committees, coordination councils, WHO and UNICEF [5].
IDD are still major public health problems in deve–loping countries although significant progress has been made towards their control strategies [6]. Historically, the territory of Ukraine is considered an endemic region for IDD. The interest to the problem of IDD in Ukraine has increased in recent years, at the same time the pre–valence of thyroid diseases among the adult population, high incidence of temporary and permanent disability is also increasing [7]. The absolute number of cases of thyroid diseases in Ukraine over the past 10 years has increased from 689,000 to 1,486,000, according to the prevalence rates, that is 941.6 and 4,210.4 cases per 100,000 of population, respectively [8]. The thyroid gland pathology with its total frequency in the population (as of 01.01.2018) is 46 % of the total endocrinological morbidity and takes the first place among endocrinopathies [9] (Fig. 1).
/542-1.jpg)
The high incidence of thyroid diseases in Ukraine is caused by many reasons, among which the main ones are the lack of iodine in the diet of the population, the imba–lance of the trace elements and vitamins composition in the diet due to the environmental degradation, the man-made pollution of the environment and inadequate preventive measures, the cessation of centralized iodine prophylaxis on the governmental level [10].
ID is a global problem for all of mankind, so studying the problem of thyroid protection is important. Epidemiological research is needed to establish the presence of ID in a particular region or country [11, 12].
National studies, which were conducted in 2002 and 2007 by V.P. Komisarenko Institute of Endocrinology and Metabolism of the National Academy of Medical Sciences of Ukraine, the Institute of Labour Medicine of the Academy of Medical Sciences of Ukraine and the UN Children’s Fund with the support of WHO proved the urgency of the ID problem for the entire territory of Ukraine [13]. The ID of varying severity is common throughout the country. So-called cluster studies were carried out to obtain a reliable assessment of the situation with the ID in a given area. For many regions, IDD is of the mild form, moderate IDD is in the northern, some central and southern regions, and severe form occurs in the western regions of Ukraine [14]. However, there is still no national IDD prevention and monitoring program in the country.
The purpose of the work was to evaluate the degree of ID, the prevalence of thyroid diseases in the population of the Western region of Ukraine, and provide a theoretical justification for developing ways to further overcome IDD.
Materials and methods
Epidemiological criteria for determining the pre–sence of ID in a particular geographical area were deve–loped and approved by WHO and UNICEF (last revised in 2018). Urinary iodine is a sensitive marker of recent dietary iodine intake; a spot urine sample is generally recommended for population-based studies [15, 16]. The iodine status study of the population in the region within the framework of an epidemiological trial was conducted among the representative samples residing in Ternopil: pregnant women (19–44 years) in the first trimester of pregnancy and children aged 12–14 years using the proportional distribution method. A sample of children for the survey included the schoolchildren (50 boys and 50 girls). The examination of children was carried out at the Ternopil Educational Complex “School of General Education I–III degrees — Medical Lyceum No 15” by the group of an endocrinologist, an ultrasound doctor, and a laboratory assistant.
The research was carried out after receiving the approval of the Ethics Commission at I. Horbachevsky Ternopil National Medical University, with the consent of the local authorities, teachers, parents and children (protocol 52, March 4, 2019). A sample of pregnant women was examined at the “Maternity Welfare Clinic of the City Maternity Hospital” in Ternopil (100 women), after receiving the approval of the Ethics Commission and their written consent. The following methods were used to define the degree of ІD: anthropometric (growth, body weight); palpation and echographic examination of the thyroid gland (using the ultrasound machine Samsung Medison R3 with a linear sensor with a frequency of 7.5 MHz); the iodine concentration was determined in a single portion of urine (60 surveyed) using the cerium-arsenic method of Sandell-Kolthoff modified in the laboratory of the Department of Epidemiology of Endo–crine Diseases of V.P. Komisarenko Institute of Endocrinology and Metabolism of the National Aca–demy of Medical Sciences of Ukraine, which is a part of the EQUIP International Program and continuously undergoes external quality control at the Center for Disease Control in Atlanta.
The results of neonatal screening of newborns for hypothyroidism from the official accounting and reporting data of the Medical Genetic Centre in Ternopil Regional Children’s Clinical Hospital were analysed.
The statistical processing of the research results was carried out using standard Microsoft Excel 2010 tools.
Results
The ID severity was assessed using the following indicators: neonatal screening of newborns for hypothyroidism, frequency of goitre found by palpation and ultrasound scan examination of the thyroid gland, and median urinary iodine. For each of these criteria, the thresholds are indicated, the epidemiological framework of the researches used for determining the ІD degrees is developed [16, 17].
The concentration of thyroid-stimulating hormone (TSH) in neonatal blood is a valuable indicator of iodine deficiency; since 2007 according to WHO/UNICEF/ICCIDD standards, an additional criterion of IDD severity in the population is the frequency of neonatal hyperthyrotropinemia (NHT). The TSH level over 5 mIU/l according to neonatal screening for congenital hypothyroidism reflects the state of iodine population availability along with such data as the frequency of goitre according to the ultrasound scan of the thyroid gland of students and the excretion of iodine in urine [18].
With adequate iodine availability, the incidence of TSH elevations over 5 mIU/l should not exceed 3 %. For mild iodine deficiency, this figure is 3–19.9 %, for mo–derate iodine deficiency — 20–39.9 %, for severe — 40 % or more. An increase in the TSH level over 5 mIU/l is defined as NHT [19]. An increase in TSH concentration over 20 mIU/l is interpreted as transient neonatal hypothyroidism as a result of violation caused by the adaptation of the pituitary-thyroid system in newborns [20]. The results of the prenatal screening are not highly reliable and they are only conditionally positive. If the screening in a newborn revealed the quantitative deviations from the reference values, additional biochemical and genetic tests were performed to confirm the presence of a dangerous disease.
A comparative analysis of the official accounting and reporting statistical data of the Medical Genetic Centre of the Ternopil Regional Children’s Clinical Prenatal Hospital for the last five years (2014–2018) has been conduc–ted. During these years, 56,713 newborns were screened. That is 98.6 % of the total live births. The coverage rate varied from 93.1 to 100 % in various regions of Ternopil. According to the results of the screening, the final diagnosis of congenital hypothyroidism was established in 8 cases for the last five years. In 2014, a significant increase in TSH (> 20 mIU/l) was observed only in 0.5 % of cases (57/11,463), that means, neonatal transient hypothyroidism was recorded. The value of TSH in the context of neonatal hyperthyrotropinemia (5–20 mIU/l) was found in 389 of 11,463 (3.4 %) infants, that according to WHO criteria meets the mild degree of iodine deficiency. In 2015, neonatal transient hypothyroidism was observed in 0.31 % of cases (41/13,368), and 2.8 % (367/13,136) of infants presented with neonatal hyperthyroidism. In 2016 and 2017, a mild degree of iodine deficiency was observed in 4.6 and 3.1 % of cases, neonatal hyperthyroidism was found in 412/8,962 and 414/13,368 infants, respectively. In 2018, neonatal transient hypothyroi–dism was detected in 0.64 % of cases, and neonatal hyperthyrotropinemia was observed in 362/9,784 (3.7 %) cases. The mean concentration of TSH was higher than the threshold and was 11.8 ± 2.0 mIU/l. The analysis of the data of the screening showed the results to exceed the normative values and correspond to a mild degree of iodi–ne deficiency in the Ternopil region.
The most important epidemiological indicator of the IDD prevalence is the incidence of goitre. Iodine deficiency is considered proven if the incidence of goitre exceeds 5 % of the examined children, according to the WHO/ICCIDD criteria (2007) [20].
The results of the palpation examination of the thyroid gland of schoolchildren demonstrated a presence of goitre I degree in 15 % of the surveyed, II degree in 9 %. The palpatory method for evaluating the thyroid carcinoma is subjective, and the ultrasonographic determination of its vo–lume is more accurate [20]. Increased thyroid gland reflects a long process of iodine intake over months and years. Today, in assessing the thyroid volume in children in epidemiological studies, the standards used take into account the area of the body surface of a child by the normogram. The analysis of the ultrasound results showed a significant increase in the incidence of thyroiditis in the examined children. The goitre was noted in 16 % of boys and in 22 % of girls. The conducted research showed a high prevalence of goitre among schoolchildren in Ternopil. In the overall calculation, the incidence of goitre by the results of thyroid ultrasound in schoolchildren reached 38 %, that is retrospectively indicated a severe degree of the ID.
According to international standards, via using thyroid ultrasound scores in women, the thyroiditis is diagnosed, if the thyroid gland volume exceeds 18 cm3, the calculation of the volume of particles was carried out according to the formula for calculating the volume of the ellipsoid [20]. According to our data, in 23 % of pregnant women in the first trimester, the thyroid parameters in goitre I degree were at the upper values of the norm (18.2 ± 1.3 cm3). In 13 % of pregnant women, the thyroid volume was within the limits (25.6 ± 1.2 cm3). Accor–ding to the results of the ultrasound examination, 36 % of pregnant women have increased thyroid gland. Ternopil belongs to a region with severe iodine deficiency, and these indicators should be considered as initial forms of IDD, that requires timely prevention and treatment.
Today the assessment of the iodine consumption in the region is guided by the urinary excretion of iodine (ioduria), which is considered as the main epidemiological indicator since 80–90 % of the consumed iodine is excreted in the urine [21, 22].
In accordance with the epidemiological criteria for school-age children, median ioduria under 20 μg/l is considered to be inadequate and iodine deficiency is severe; at median ioduria 20–49 μg/l, iodine intake is considered insufficient and iodine deficiency is modera–te; at median ioduria 50–99 μg/l, iodine intake is considered insufficient and iodine deficiency is mild. At the same time, if the median urinary concentration of iodine exceeds 100 μg/l, this indicates iodine deficiency in a particular population. At median ioduria 100–199 μg/l, iodi–ne intake is considered normal, and iodine availabi–lity is optimal; with median ioduria 200–299 μg/l, iodine intake is considered to be more necessary, and iodine provision can create a negligible risk of over-consumption for the entire population; with median ioduria more than or equal to 300 μg/l, iodine intake is considered excessive, there is a risk of adverse health effects [21].
In 50 % of the examined children of school age (12–14 years), the urinary concentration of iodine averaged 163.26 μg/l, which indicates the optimal supply of children with iodine (Fig. 2).
/544-1.jpg)
Inadequate iodine supplementation was observed in 20 % of children at risk of iodine deficiency with a range of 23.59 to 91.53 μg/l. A mild iodine deficiency was detected in 13 % and moderate in 7 % of children. Excessive iodine intake was observed in 20 % of children with median ioduria over 250 μg/l. In 10 % of the examined children, the median ioduria value fluctuated around an average 476.01 μg/l, indicating the danger of negative consequences (Fig. 3). With such long-term consumption, a chronic excess of iodine in the body may develop with increased thyroid volume and autoimmune diseases (autoimmune thyroiditis, thyrotoxicosis and other pathologies).
During the gestation, in the body of a pregnant wo–man there is an increase in renal blood flow and glomerular filtration, which is accompanied by additional loss of iodine in the urine and an increase in the need for this micronutrient, that is why the median for ioduria in pregnant women is doubled [22]. According to the current recommendations of the International Council for the Control of IDD (ICCIDD), the optimal level of ioduria during pregnancy is defined as a range of 150–230 μg/l, iodine intake by pregnant women is not sufficient for median iodine level under 150 μg/l, is more needed at 230–499 μg/l, and is excessive in iodine concentration ≥ 500 μg/l [23].
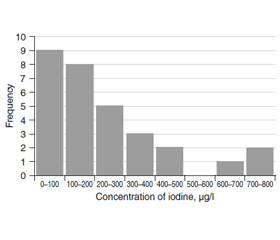
Inadequate iodine supplementation was observed in 43.3 % of the examined pregnant women, median ioduria was on average 81.96 μg/l with a range of 26.53 to 135.87 μg/l. This situation leads to excessive chronic thyroid stimulation, hyperplasia of the thyroid gland and possible adverse effects on the physical development and the state of the central nervous system of the fetus and the child, with the formation of reduced criteria for congenital intelligence and mental retardation at all stages of the further life [24] (Fig. 4).
/544-2.jpg)
In 26.7 % of pregnant women, the urinary concentration of iodine corresponded to the normal range (150–230 μg/l) and averaged 175.29 μg/l. Excessive iodi–ne intake, with median above 230 μg/l, was detected in 30 % of pregnant women. Of these, 10 % of women had iodine median higher than 500 μg/l with a range of 682.77 to 791.03 μg/l, indicating excessive iodi–ne intake (Fig. 5).
Discussion
The state of the iodine supply in the Ternopil region according to the results of the neonatal screening for congenital hypothyroidism corresponds to a mild degree of iodine deficiency in the population (the frequency of neonatal hyperthyrotropinemia was 3.52 ± 0.30 %), the mean concentration of TSH was higher than the thres–hold and was 11.8 ± 2.0 mIU/l.
The incidence rate of the goitre in the selected refe–rence group of students is 38 % by the results of the ultrasonographic examination of the thyroid gland and 36 % for pregnant women, that indicates severe iodine deficiency in the region as a whole.
The values of the median of ioduria in school-age children showed a low iodine supplement in 20 % of children (a mild iodine deficiency in 13 % and a mode–rate form in 7 %), the urinary concentration of iodine was on average 99.69 ± 35.42 μg/l. Thirty per cent children presented with an excessive iodine intake over 250 μg/l and 50 % of the examined children had an optimal iodine content of 163.26 μg/l on average.
Low iodine diet in pregnant women and the lack of adequate individual iodine prophylaxis manifested by a low median of iodine. In 43.3 % of the exami–ned pregnant women, the median of ioduria averaged 81.96 ± 42.53 μg/l. In 26.7 % of pregnant women, the urinary concentration of iodine corresponded to normal intervals and excessive iodine intake, with a median above 230 μg/l, was detected in 30 % of pregnant women.
In women with a long history of iodine intake and a rapid increase in iodine intake during pregnancy, there is a potential risk of iodine hyperthyroidism and other pathologies [23]. For adequate iodine provision for pregnant women, it is necessary to monitor the iodine intake in the form of iodized salt and iodine preparations with a control of thyroid hormonal status and the urinary concentration of iodine [26]. Consequently, the epidemiological data on iodine maintenance in population from the Ternopil region demonstrate a severe degree of ID that requires urgent preventive measures to overcome the ID in high-risk groups, which include children and women of reproductive age (including pregnant wo–men). In the absence of a state legislative framework for the ID prevention, an alternative is the introduction of individual prevention of IDD.
Conclusions
Received epidemiological data of estimation of iodine maintenance in the population of the Western region of Ukraine correspond to the severe degree of iodine deficiency at the population level according to the results of ultrasonographic examination of thyroid gland; in the third part of the surveyed, the urinary concentration of iodine demonstrated the insufficient iodine maintenance of moderate degree. These iodine deficiency indicators require the implementation of an urgent national program for IDD prevention in high-risk groups, which include children and women of reproductive age (including pregnant women). In the absence of a legislative framework for the prevention of iodine deficiency in Ukraine, the introduction of mass prophylaxis at the state level is an alternative, based on the experience of neighbouring European countries.
Conflicts of interests. Authors declare the absence of any conflicts of interests and their own financial interest that might be construed to influence the results or interpretation of their manuscript.