Резюме
Вірус Епштейна — Барр (ВЕБ) вражає 9 із 10 осіб в якийсь момент їх життя. Хоча зазвичай перебіг інфекції сприятливий, вона може проявлятися безліччю симптомів й ускладнень. Ми наводимо випадок ВЕБ у раніше здорового 21-річного чоловіка, у якого протягом 8 днів спостерігалися дисфагія, фарингіт, кашель, болі в животі і стомлюваність, а раніше також підвищувалася температура, що досягала максимального значення 38,5 °С. При клінічному огляді відзначено тільки хворобливість живота. Під час госпіталізації з приводу ВЕБ у пацієнта раптово виникла ниркова недостатність, що спостерігалася протягом 4 днів, швидкість клубочкової фільтрації знизилася до 33 мл/хв/1,73 м2, а згодом довільно відновилася до нормального рівня. Це сталося лише при підтримуючому лікуванні без застосування кортикостероїдів. Даний випадок ілюструє атиповий перебіг інфекції ВЕБ і становить собою приклад спонтанної нормалізації функції нирок.
Вирус Эпштейна — Барр (ВЭБ) поражает 9 из 10 человек в какой-то момент их жизни. Хотя обычно течение инфекции благоприятное, она может проявляться множеством симптомов и осложнений. Мы представляем случай ВЭБ у ранее здорового 21-летнего мужчины, у которого в течение 8 дней наблюдались дисфагия, фарингит, кашель, боли в животе и утомляемость, а ранее также повышалась температура, достигавшая максимального значения 38,5 °С. При клиническом осмотре отмечена только болезненность живота. Во время госпитализации по поводу ВЭБ у пациента внезапно возникла почечная недостаточность, наблюдавшаяся в течение 4 дней, скорость клубочковой фильтрации снизилась до 33 мл/мин/1,73 м2, а впоследствии произвольно восстановилась до нормального уровня. Это произошло лишь при поддерживающем лечении без применения кортикостероидов. Данный случай иллюстрирует атипичное течение инфекции ВЭБ и представляет собой пример спонтанной нормализации функции почек.
Epstein-Barr virus (EBV) affects 9 out of 10 people at some point in their lives. Though generally a benign infection, it can present with a plethora of symptoms and complications. We present the case of a 21-year-old previously healthy male suffering from EBV who presented with an 8-day history of odynophagia, pharyngitis, cough, abdominal pain and fatigue, previously he also had a fever which reached a maximum of 38.5 °C. The patient’s clinical exam was positive only for abdominal tenderness. During his hospitalisation for EBV, our patient suffered sudden renal failure over the course of 4 days, with a glomerular filtration rate dropping to 33 mL/min/1.73 m2, before spontaneously recovering to normal levels. This occurred with supportive treatment only and without the use of corticosteroids. This case illustrates an atypical presentation of EBV infection and provides a further example of spontaneous recovery of renal function.
Introduction
Epstein Barr virus (EBV), responsible for mononucleosis, is one of the world’s most common human viruses, with 9 out 10 people worldwide having been infected [1]. Patients typically present with pharyngitis, cervical lymphadenopathy, fatigue, anorexia, fever and upper respiratory symptoms and, rarely, abdominal pain [1]. The acute illness lasts for around 3 weeks, with spontaneous recovery thereafter [1].
The most common routes of transmission are kissing and sexual intercourse, though it also possible to be infected by contaminated blood or organ transplants [1].
Though usually benign, around 1 % of patients present with complications, which may be serious or even life threatening [1]. The complications include but are not limited to; haemolytic anaemia, thrombocytopenia, splenomegaly, meningoencephalitis, cholecystitis or pharyngeal obstruction, though any organ system can be affected [1, 2]. However, rare cases of acute renal failure secondary to EBV infections have been reported in the literature, with references to renal involvement being reported as far back as 1889 when first described by E. Pfeiffer, at which time it was referred to as glandular fever [2, 3].
We present a case of a 21-year-old man with a rapid and unexpected decline in renal function during a hospitalisation, following a recent EBV infection.
Case presentation
Our patient presented to the emergency department (ER) following an 8-day history of odynophagia, pharyngitis, cough, abdominal pain, and fatigue. He also reported a low-grade fever that lasted for 4 days at the start of the episode and a single episode of vomiting. He had been self-medicating with ibuprofen and paracetamol before presenting to the ER but did not habitually take any medications. His medical history was unremarkable. His vitals were as follows; temperature was 36.3 °C, blood pressure 118/61 mmHg, pulse 100 bpm and 100 % oxygen saturation. His physical examination revealed a tenderness in both the hypogastric and right hypochondral regions with no palpable organomegaly, with the rest of his exam being unremarkable.
No PCR for EBV was performed. The diagnosis was made clinically due to the patient having highly suggestive symptoms and history, with the addition of IgG (242 U/ml) and borderline positive IgM levels, which we interpreted as being recovery from an initial infection ( his symptoms having started a week before the blood test/antibody serology was performed).
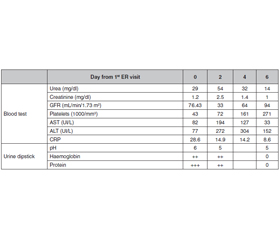
The patient had presented to the ER two days prior with a 38.5 °C fever. A non-contrast CT-scan was performed, which was unremarkable. A blood test was performed, visible in table 1 as day 0. His blood test revealed a thrombocytopenia of 43 000/mm3, a low white blood cell count of 4 300/mm3, ALT 82 U/L, ALT 77 U/L, CRP 28.6 mg/L, creatinine of 1.2 mg/dL, and an estimated creatinine clearance rate of 76.43 mL/min/1.73m2. He also had a mild hyponatraemia at 133 mmol/L and hypochloraemia at 92.4 mmol/L.
/108.jpg)
Upon his second presentation two days later he still had a thrombocytopenia at 71 000/mm3, a recovered white blood cell count of 6 100/mm3, worsened liver tests of ALT 194 U/L, ALT 272 U/L, and an improved CRP 14.9 mg/L. His kidney function, however, had rapidly degraded with a creatinine of 2.5 mg/dL and an estimated creatinine clearance rate of 33 mL/min/1.73 m2. He remained hyponatraemic and hypochloraemic with 127 mmol/L and 89 mmol/L respectively. Anti-nuclear antibodies (ANA) and antineutrophil cytoplasmic antibodies (ANCA) were tested to rule out an auto-immune origin, with both returning negative results. A urine dipstick was performed, revealing a pH of 5, 2 crosses of protein and 2 crosses of haemoglobin, with no signs of a urinary tract infection.
Two days following admission, the patient’s renal tests spontaneously began to improve, and he required no further treatment. Due to the improvement in renal function, a renal biopsy was not performed.
On the 6th day of hospitalisation, the patient was discharged, having fully recovered.
Discussion
EBV, the causative agent of mononucleosis, is generally self-limiting and typically presents with a triad of fever, pharyngitis and cervical adenopathy, though complications may occur and involve other organ systems [1].
When our patient presented at the emergency department it is likely that they had already been ill for some time as the IgM to IgG shift had already occurred, with hepatic and renal involvement also present.
Our patient presented with both typical and atypical signs of EBV infection, having had the typical fever, pharyngitis, fatigue, and hepatic enzyme elevation with the atypical signs being abdominal pain, and acute renal failure. Notably, we observed no cervical adenopathy.
Previous studies of students of similar ages to our patient also found most patients suffered from pharyngitis, pyrexia and cervical adenopathy, with less than half suffering from cough and only 15 % presenting with abdominal pain [1]. Other studies found haematuria and proteinuria in 11 and 14 % of patients respectively, making it an even rarer occurrence, our patient presenting with both simultaneously [4].
Although our patient had taken ibuprofen and vomited once, we do not believe this caused the renal failure as it progressed in the days following hospitalisation at which time the medication has been stopped and the patient rehydrated. We also believe that the presence of protein and blood in the urine dipstick pleads against simple dehydration being the cause of the renal failure.
The physiopathology of EBV associated kidney failure is thought to result from interstitial nephritis with two possible explanations being put forward [5]. The first of these suggests that the kidney is subject to an attack by T-lymphocytes targeting infected lymphocytes presenting EBV antigens which are passing through it [5]. The second hypothesis is that EBV directly infects renal cells, causing an auto-immune response against the infected cells, resulting in the kidney damage and subsequent failure [4]. Case reports of EBV related kidney failure in which biopsies were performed, though heterogenous in nature, revealed interstitial infiltrates without much glomerular involvement [5].
The patient very briefly presented with mild anemia a few days after admission and at one point had slightly elevated conjugated bilirubin. We did not make a clinical diagnosis of anemia.
We did not consider HUS as a possible diagnosis due to the lack of a history of diarrhea and the anemia being very mild and transient.
Corticosteroids use can be found in many case reports, with some finding that there is marked improvement after administration, though others note that their use is debatable for the treatment of EBV in general, as well as in the context of EBV induced renal failure [1, 2, 6]. Our patient recovered spontaneously within 5 days, lending more credence to the argument that treatment may not be necessary. As this was the case, no renal biopsies were taken.
Conclusions
In conclusion, this case is an example of an uncommon complication of EBV. Though the acute renal failure may be rapid, it does not necessarily require treatment and in some cases, patients can fully recover with only supportive care.
Received 28.07.2021
Revised 08.08.2021
Accepted 09.08.2021
Список литературы
1. Dunmire S.K., Verghese P.S., Balfour H.H. Primary Epstein-Barr virus infection. Journal of Clinical Virology. Elsevier B.V. 2018. Vol. 102. Р. 84-92.
2. Kien C., Ganta K. An Atypical Presentation of Epstein-Barr Virus Associated Infectious Mononucleosis Mistaken for Pyelonephritis. Cureus [Internet]. 2020, Apr 8 [cited 2021, Jun 20]. 12(4). Available from: /pmc/articles/PMC7212761/.
3. Tidy H.L., Morley E.B. Glandular fever. Br. Med. J. [Internet]. 1921, Apr 18 [cited 2021, Jun 20]. 1(3143). 452-456. Available from: https://www.bmj.com/content/1/3143/452.
4. Dylewski J., Roy I., Eid J. Acute renal failure associated with acute epstein-barr virus infection. Infect. Dis. Clin. Pract. [Internet]. 2008 Mar [cited 2021, Jun 20]. 16(2). 127-128. Available from: https://journals.lww.com/infectdis/Fulltext/2008/03000/Acute_Renal_Failure_Associated_With_Acute.13.aspx.
5. Mayer H.B., Wanke C.A., Williams M., Crosson A.W., Federman M., Hammer S.M. Epstein-Barr Virus-Induced Infectious Mononucleosis Complicated by Acute Renal Failure: Case Report and Review [Internet]. 1996 [cited 2021, Jun 20]. Available from: https://academic.oup.com/cid/article/22/6/1009/465411.
6. Lei P.S., Lowichik A., Allen W., Mauch T.J. Acute renal failure: Unusual complication of Epstein-Barr virus-induced infectious mononucleosis. Clin. Infect. Dis. [Internet]. 2000, Dec 1 [cited 2021, Jun 20]. 31(6). 1519-1524. Available from: https://academic.oup.com/cid/article/31/6/1519/373063.

/108.jpg)