
Международный эндокринологический журнал Том 17, №5, 2021
Вернуться к номеру
Оцінка факторів, що впливають на стан пацієнта після баріатричної хірургії
Авторы: Marisol Barradas-Lagunes, Paola Bravo-De Avila, Raquel Colorado-Subizar, Maripi De Uriarte-Llorente, Rosario Gamboa-Huerta, Rey Jesus Romero
Bariatric and Metabolic Surgery Center Obesity Health, Boca del Río, Veracruz, México
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
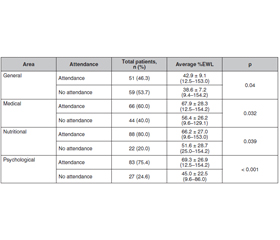
Вступ. Програми баріатричної хірургії визнані найкращою альтернативою для пацієнтів із морбідним ожирінням. У багатьох дослідженнях дійшли висновку, що програми баріатричної хірургії, які містять до- та післяопераційні консультації спеціалістів багатопрофільної команди, мають кращі загальні результати. Метою даного дослідження була оцінка факторів, що впливають на до- та післяопераційні консультації спеціалістів під час програми баріатричної хірургії в Мексиці, та оцінка їх можливого впливу на післяопераційний курс реабілітації пацієнтів. Матеріали та методи. Відповідно до настанови Міжнародної федерації хірургічного лікування ожиріння і метаболічних розладів (IFSO), усі пацієнти на час проведення баріатричної операції мали вік від 18 до 65 років. Передопераційна оцінка показань пацієнтів до баріатричної хірургії містила консультації з оперуючим хірургом, дієтологом, терапевтом та психологом. За умов виявлення протипоказань чи наявності супутніх захворювань дані питання розглядалися до прийняття рішення про проведення операції. Результати. Усього в дослідження були включені 110 пацієнтів. З цього числа жінки становили 81 особу (74 %) і 29 (26 %) — чоловіки. Установлено, що жінки отримували консультації спеціалістів вірогідно частіше, ніж чоловіки (54,3 проти 24,1 %, p = 0,005). Пацієнти з вищим початковим індексом маси тіла відвідували спеціалістів вірогідно частіше, ніж пацієнти з нижчим індексом маси тіла (42,9 проти 38,6 кг/м2, р = 0,007). При оцінці частоти консультацій за професією хворих педагогічні працівники вірогідно частіше (p = 0,003) відвідували спеціалістів багатопрофільної команди (71,4 %), тоді як студенти рідше відвідували суміжних спеціалістів. Пацієнти, які мали більший відсоток перевищення маси (EWL), вірогідно частіше відвідували спеціалістів із питань харчування, способу життя та психологічних аспектів, ніж пацієнти з меншим відсотком EWL (p < 0,001). Висновки. Проведення консультацій спеціалістами багатопрофільної команди асоціюється з кращими результатами після баріатричної операції. У пацієнтів, яким такий огляд не проводився, частіше спостерігаються неоптимальні результати. При проведенні таких консультацій слід також зважати на культурні, соціальні, економічні та мотиваційні причини з боку пацієнтів.
Background. Bariatric surgery programs are recognized as the best alternative for patients with severe obesity. Many studies conclude that bariatric surgery programs that include these pre- and postoperative consultations (PPC) by the multidisciplinary team have better overall outcome. The purpose of the present study was to evaluate factors that affect PPC during a bariatric surgery program in Mexico and assess the possible impact on the patients’ post-operative course. Materials and methods. In accordance with the the International Federation for the Surgery of Obesity and Metabolic Disorders guidelines, all patients included were between 18 and 65 age when bariatric surgery was performed. Preoperative assessment of patient eligibility for bariatric surgery included consultation with the main surgeon, a dietician, an internist, and a psychologist. If non-eligible cases were detected, these issues were addressed and fully treated before surgery was considered. Results. A total of 110 patients were included in this study. Eighty-one (74 %) patients were women and 29 (26 %) were men. We observed that women had significantly more consultation attendance than men (54.3 % versus 24.1 %, p = 0.005). Patients with higher initial BMI had significantly more consultation attendance than those with lower BMI (42.9 kg/m2 versus 38.6 kg/m2, p = 0.007). When consultation attendance was evaluated according to occupation, teaching workers had significantly (p = 0.003) more consultation attendance (71.4 %) while the students group had less consultation attendance (0). Patients who had higher percentage of excess of weight loss (EWL) had significantly more general, medical, nutritional and psychological consultation attendance than those with lower percentage of EWL (p = 0.04, p = 0.032, p = 0.039 and p < 0.001). Conclusions. Consultation attendance with the multidisciplinary team is associated with better outcomes after bariatric surgery. “Nonattending” patients are at least partly responsible for any suboptimal results observed. Although this is certainly a factor for some patients, many other non-dependent reasons, such as cultural, social, economic or motivational reasons can also affect the loss of consultations in other patients.
баріатрична хірургія; консультації спеціалістів; багатопрофільна команда; оцінка факторів
bariatric surgery; consultation attendance; multidisciplinary team; assessment of factors
Introduction
Material and methods
Results
/29.jpg)
/30.jpg)
Discussion
Conclusions
- Magno F.C., Silva M., Cohen L., Sarmento L., Rosado E. Nutricional profile of patients in a multidisciplinary treatment program for severe obesity and preoperative bariatric surgery. Abcd. Arq. Bras. Cir. Dig. 2014. 27. 31-34. https://doi.org/10.1590/s0102-6720201400s100008.
- Lundin K.I., Bergh I., Von Soest T., Rosenvinge J.H. A comparison of behavioral and psychological characteristics of patiens opting for surgical and conservative treatment for morbid obesity. BMC Obesity. 2016. 3. 6. https://doi.org/10.1186/s40608-016-0084-6.
- Golubic R., Laur C., Kelsey M., Livesy A., Hoensch J., Park A. The Cambridge Intensive Weight Management Program Appears to Promote Weight Loss and Reduce the Need for Bariatrics Surgery in Obese Adults. Frontiers in Nutrition. 2018. 5. 54. https://doi.org/10.3389/fnut.2018.00054.
- Unick J.L., Beavers D., Bond D.S., Clark J.M., Jakicic J.M., Kitabchi A.E., Knowler W.C. et al. Look AHEAD Research Group. The long-term effectiveness of a lifestyle intervention in severely obese individuals. Am. J. Med. 2013. 126. 236-242. https://doi.org/10.1016/j.amjmed.2012.10.010.
- Hsu L.K., Benotti P.N., Dwyer J., Roberts S.B., Saltzman E., Shikora S., Rolls B.J., Rand W. Nonsurgical factors that influence the outcome of bariatric surgery: a review. Psychosom. Med. 1998. 60. 338-346. https://doi.org/10.1097/00006842-199805000-00021.
- O’Kane M., Parretti H.M., Hughes C.A., Sharma M., Woodcock S., Puplampu T., Blakemore A.I. et al. Guidelines for the follow-up of patients undergoing bariatric surgery. Clin. Obes. 2016. 6. 210-224. https://doi.org/10.1111/cob.12145.
- Khorgami Z., Zhang C., Messiah S.E., de la Cruz-Muñoz N. Predictors of Postoperative Aftercare Attrition among Gastric Bypass Patients. Bariatr. Surg. Pract. Patient Care. 2015. 10. 79-83. https://doi.org/10.1089/bari.2014.0053.
- Mechanick J.I., Youdim A., Jones D.B., Garvey W.T., Hurley D.L., McMahon M.M., Heinberg L.J. et al. American Association of Clinical Endocrinologists; Obesity Society; American Society for Metabolic & Bariatric Surgery. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient — 2013 update: cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Endocr. Pract. 2013. 19. 337-372. https://doi.org/10.4158/EP12437.GL.
- Belo G.Q.M.B., Siqueira L.T., Melo Filho D.A.A., Krei-mer F., Ramos V.P., Ferraz Á.A.B. Predictors of poor follow-up after bariatric surgery. Rev. Col. Bras. Cir. 2018. 45. e1779. https://doi.org/10.1590/0100-6991e-20181779.
- Vidal P., Ramón J.M., Goday A., Parri A., Crous X., Trillo L., Pera M., Grande L. Lack of adherence to follow-up visits after bariatric surgery: reasons and outcome. Obes. Surg. 2014. 24. 179-183. https://doi.org/10.1007/s11695-013-1094-9.
- Jennings N., Boyle M., Mahawar K., Balupuri S., Small P. The relationship of distance from the surgical centre on attendance and weight loss after laparoscopic gastric bypass surgery in the United Kingdom. Clin. Obes. 2013. 3. 180-184. https://doi.org/10.1111/cob.12031.
- Perez-Lugo A.L., Gabino-Campos M., Baile J.I. Analysis of the aesthetic stereotypes of women in nine fashion and beauty mexican magazines. Rev. Mex. Trastor. Alimen. 2016. 7. 40-45. https://doi.org/10.1016/j.rmta.2016.02.001.
- Compher C.W., Hanlon A., Kang Y., Elkin L., Williams N.N. Attendance at clinical visits predicts weight loss after gastric bypass surgery. Obes. Surg. 2012. 22. 927-934. https://doi.org/10.1007/s11695-011-0577-9.
- Vilallonga R., Lecube A., Fort J.M., Boleko M.A., Hidalgo M., Armengol M. Internet of things and bariatric surgery follow-up: Comparative study of standard and IoT follow-up. Minim. Invasive Ther. Allied Technol. 2013. 22. 304-311. https://doi.org/10.3109/13645706.2013.779282.
- Greenhalgh T., Vijayaraghavan S., Wherton J., Shaw S., Byrne E., Campbell-Richards D., Bhattacharya S. et al. Virtual online consultations: advantages and limitations (VOCAL) study. BMJ Open. 2016. 6. e009388. https://doi.org/10.1136/bmjopen-2015-009388.
- El Chaar M., McDeavitt K., Richardson S., Gersin K.S., Kuwada T.S., Stefanidis D. Does patient compliance with preoperative bariatric office visits affect postoperative excess weight loss? Surg. Obes. Relat. Dis. 2011. 7. 743-748. https://doi.org/10.1016/j.soard.2010.10.020.
- Shen R., Dugay G., Rajaram K., Cabrera I., Siegel N., Ren C.J. Impact of patient follow-up on weight loss after bariatric surgery. Obes. Surg. 2004. 14. 514-519. https://doi.org/10.1381/096089204323013523.
- Dixon J.B., Laurie C.P., Anderson M.L., Hayden M.J., Dixon M.E., O’Brien P.E. Motivation, readiness to change, and weight loss following adjustable gastric band surgery. Obesity (Silver Spring). 2009. 17. 698-705. https://doi.org/10.1038/oby.2008.609.
- Weichman K., Ren C., Kurian M., Heekoung A.Y., Casciano R., Stern L., Fielding G. The effectiveness of adjustable gastric banding: a retrospective 6-year U.S. follow-up study. Surg. Endosc. 2011. 25. 397-403. https://doi.org/10.1007/s00464-010-1178-8.
- Tess B.H., Scabim V.M., Santo M.A., Pereira J.C. Obese patients lose weight independently of nutritional follow-up after bariatric surgery. Rev. Assoc. Med. Bras. (1992). 2015. 61. 139-143. https://doi.org/10.1590/1806-9282.61.02.139.
- Rutledge T., Groesz L.M., Savu M. Psychiatric factors and weight loss patterns following gastric bypass surgery in a veteran population. Obes. Surg. 2011. 21. 29-35. https://doi.org/10.1007/s11695-009-9923-6.
- Sarwer D.B., Moore R.H., Spitzer J.C., Wadden T.A., Raper S.E., Williams N.N. A pilot study investigating the efficacy of postoperative dietary counseling to improve outcomes after bariatric surgery. Surg. Obes. Relat. Dis. 2012. 8. 561-568. https://doi.org/10.1016/j.soard.2012.02.010.
- Kolotkin R.L., Andersen J.R. A systematic review of reviews: exploring the relationship between obesity, weight loss and health-related quality of life. Clin. Obes. 2017. 7. 273-289. https://doi.org/10.1111/cob.12203.
- Gould J.C., Beverstein G., Reinhardt S., Garren M.J. Impact of routine and long-term follow-up on weight loss after laparoscopic gastric bypass. Surg. Obes. Relat. Dis. 2007. 3. 627-630; discussion 630. https://doi.org/10.1016/j.soard.2007.07.005.