Вступ
Диспластичний коксартроз у дорослих пацієнтів характеризується цілою низкою особливостей. Насамперед це зміна геометричних параметрів, проксимального відділу стегнової кістки, вертлюжної западини та їх співвідношень. Зокрема, у пацієнтів із цією патологією часто спостерігається збільшення шийково-діафізарного кута (ШДК) стегнової кістки, змінюється форма вертлюжної западини, її глибина, товщина її дна, співвідношення проксимального відділу стегнової кістки та вертлюжної западини [1–4], тобто порушується конгруентність суглобових поверхонь.
При зміненні геометричних параметрів кульшового суглоба змінюються кути прикріплення м’язів та плечі їх сил, що обумовлює особливості роботи м’язів тазового пояса. Зокрема, зміна кута прикріплення м’яза або кута його дії разом із вкороченням плеча сили м’яза призводять до зменшення моменту сили, що знижує ефективність його роботи. Крім того, самі м’язи в дорослих пацієнтів із диспластичним коксартрозом під час прогресування захворювання розвиваються інакше, ніж у нормальних умовах, тому їх скорочувальна активність й абсолютна сила нижчі. Розвиток в цих умовах згинально-привідної контрактури з м’язовим дисбалансом і порушенням рухів у кульшовому суглобі також негативно впливає на роботу м’язового апарата тазового пояса [5], зменшуючи ефективність роботи абдукційного механізму.
Клінічне дослідження роботи м’язів тазового пояса має певні обмеження [6] і не дозволяє повноцінно вивчити, як робота м’язів залежить від геометричних параметрів кульшового суглоба, тому моделювання роботи м’язів тазового пояса було обрано нами як інструмент для вивчення ефективної роботи абдукційного апарата кульшового суглоба. В основу розробки такої моделі покладено принцип горизонтальної рівноваги таза при одноопорному стоянні, тобто м’язи-абдуктори стегна повинні протидіяти вазі пацієнта (силі гравітації), утримуючи таз горизонтально не менш ніж із двократним запасом міцності. Це так звана робота абдукційного механізму, ефективність якої клінічно ми оцінюємо за наявності кульгавості при ходьбі, ознак Тренделенбуга та Дюшена, використання додаткових опор тощо.
Мета роботи — обґрунтування та побудова математичної моделі роботи м’язів тазового пояса при диспластичному коксартрозі.
Матеріали та методи
В основу будови моделі роботи м’язів тазового пояса при диспластичному коксартрозі було покладено базову фізичну модель таза та нижньої кінцівки, розроблену в лабораторії біомеханіки ГУ «Інститут патології хребта та суглобів ім. проф. М.І. Ситенка НАМН України», на основі якої створено пласку графічну модель [7], до якої були внесені суттєві доповнення та зміни. Зокрема, були змінені геометричні параметри кульшового суглоба (збільшено ШДК стегнової кістки, потовщено дно вертлюгової западини, змінено положення центра обертання головки стегнової кістки), що призвело до зміни кутів прикріплення м’язів тазового пояса та моментів сил та інших змін. Зміну параметрів кульшового суглоба виконували згідно з даними проведеної раніше рентгенометрії 49 кульшових суглобів дорослих пацієнтів із диспластичним коксартрозом (із дисплазією кульшового суглоба I–III ступеня за Crowe, 1979 [8]). Крім того, до моделі додано привідні м’язи та змодельована згинально-привідна контрактура кульшового суглоба.
Графічна модель кульшового суглоба з позначенням м’язів — стабілізаторів таза та схеми їх дії подані на рис. 1.
На основі даної графічної моделі побудована розрахункова схема роботи м’язів у вигляді важеля першого роду (рис. 2), що відрізняється від базової розрахункової схеми показниками величини плеча сили та кутом прикріплення кожного м’яза, характерними для дисплазії кульшового суглоба, а також включає м’язи привідної групи стегна. Як і в базовій моделі, для кожного з м’язів було визначено параметри його роботи та його внесок у збереження горизонтальної рівноваги таза, складено рівняння рівноваги моментів сил м’язів тазового пояса та проаналізовано роботу всіх м’язів тазового пояса, зазначених у моделі.
Сама математична модель являє собою рівняння рівноваги моментів м’язових сил — горизонтальних стабілізаторів таза.
Рівняння рівноваги моментів сил для нашої розрахункової схеми буде мати вигляд:
або
або
де буквами a, b, c, d, e, g, h позначено величину плеча сили відповідного м’яза, а α, β, γ, φ, ϕ, θ, ε, η, λ, μ, δ — кут дії сили відповідного м’яза.
Характеристики роботи м’язів взяті з літературних даних [11] та отримані шляхом прямих вимірів на фізичній моделі (табл. 1).
Результати
Підставляючи значення ваги тіла пацієнта, величин плеча сил та кутів дії м’язів із табл. 1 в рівняння (4), отримуємо:
або
Таким чином, ми отримуємо показники сил, необхідних для збереження горизонтальної рівноваги таза в нормі (табл. 2).
Як бачимо з даних таблиці, кожен із м’язів, що забезпечують горизонтальну рівновагу таза, у нормі (при вазі пацієнта 80 кг) розвиває силу, що становить близько половини своєї максимально можливої сили, тобто всі м’язи працюють як мінімум із дворазовим запасом міцності. А якщо взяти до уваги синергізм роботи м’язів-абдукторів (підвищення поєднаної сили м’язів-агоністів під час руху), то можна говорити, що запас міцності роботи м’язів у нормі становить не менше 3–4 разів.
Натомість збільшення ваги пацієнта на 20–25 % (до 100 кг і більше) помітно погіршує ефективність роботи м’язів. Вони змушені задіяти понад 70–80 % своєї абсолютної сили, що різко знижує їх витривалість та ефективність роботи.
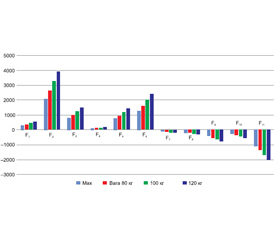
Як приклад наводимо діаграму величин сили м’язів тазового пояса, необхідної для збереження горизонтальної рівноваги таза (рис. 3).
На діаграмі чітко візуалізується, що необхідна для горизонтальної рівноваги таза сила кожного з аналізованих м’язів (другий стовпець) менша за її абсолютні значення (перший стовпець) майже вдвічі. Але збільшення ваги пацієнта на 20 % і більше (третій та четвертий стовпці) вимагає від кожного з м’язів зусиль у 70–80 % від його максимальних можливостей.
В умовах тривалого функціонування диспластичного кульшового суглоба виникає як ціла низка змін геометричних параметрів вертлюжної западини та проксимального відділу стегнової кістки, так і порушення в роботі м’язів тазового пояса.
Тому ми підставили в рівняння (4) конкретні значення змінених геометричних параметрів кульшового суглоба, характерних для диспластичного суглоба, та занижені показники абсолютної сили м’язів, що характерно для диспластичного процесу. Такими зміненими параметрами були: ШДК стегнової кістки, товщина дна вертлюжної западини, латералізація центра обертання головки стегнової кістки, величина приведення стегна. Таким чином, нам вдалося визначити вплив конкретних змінених показників кульшового суглоба на роботу м’язів тазового пояса.
Для порівняння наводимо діаграми зусиль м’язів при 1-му та 3-му типі дисплазії тазостегнового суглоба за Crowe (рис. 4, 5).
Як видно з наведеної діаграми, при легкому ступені дисплазії (1-й тип за Crowe) кожен з аналізованих м’язів (другий стовпець) розвиває силу, на третину менше її абсолютних значень (перший стовпець). За умов м’язового синергізму це можна вважати задовільною функцією м’язів. Але збільшення ваги пацієнта на 20 % (третій стовпець) вимагає від кожного з м’язів майже максимальних зусиль. А подальше збільшення ваги (четвертий стовпець) потребує зусиль, що перевищують можливості м’яза. Тобто вага пацієнта має важливий негативний вплив на роботу м’язів – горизонтальних стабілізаторів таза.
/9.jpg)
Отримані дані показують, що при тяжкому ступені дисплазії кульшового суглоба (3-й тип за Crowe) м’язи не в змозі впоратися з роботою зі збереження горизонтальної рівноваги таза. Отже, ознаки м’язової недостатності у вигляді кульгавості, розгойдування тулуба, нахилів тазу при ходьбі матимуть постійні прояви. Пацієнти змушені будуть користуватися додатковою опорою або застосовувати пристосувальні механізми для полегшення пересування, тому що від м’язів вимагатимуться зусилля, що перевищують їх можливості.
Обговорення
Таким чином, використовуючи розроблену нами модель роботи м’язів зі збереження горизонтальної рівноваги таза, ми оцінили ефективність роботи абдукційного механізму в нормі, потім, після внесення змін, характерних для диспластичного ураження кульшового суглоба, ми промоделювали внесок кожної патологічної зміни в порушення роботи абдукційного механізму. Використовуючи сукупність усіх патологічних змін, ми створили математичні моделі диспластичного коксартрозу з різним ступенем вираженості змін, які ми умовно визначили як легкі, середні та тяжкі диспластичні зміни кульшового суглоба (1–3-й типи за Crowe). Аналізуючи отримані в результаті моделювання дані про роботу м’язів диспластичного кульшового суглоба, слід зазначити, що побудована математична модель відповідає поставленим завданням, варіанти моделей 1–3-го типів за Crowe узгоджуються з клінічною картиною дисплазії кульшового суглоба різного ступеня в дорослих хворих і можуть бути використані для подальшої роботи.
Математичне моделювання роботи м’язів тазового пояса в умовах дисплазії кульшового суглоба показало, що:
— збільшення ШДК стегнової кістки негативно, але не критично впливає на ефективність роботи м’язів тазового пояса, також помірний негативний влив справляє згинально-привідна контрактура кульшового суглоба;
— потовщення дна вертлюжної западини до 5 мм не справляє вираженого впливу на роботу м’язів тазового пояса, проте подальше збільшення товщини дна вертлюжної западини різко погіршує умови роботи м’язів-абдукторів та різко знижує ефективність роботи абдукційного механізму;
— латералізація центра обертання головки стегнової кістки має набагато більший негативний вплив на роботу м’язів, ніж потовщення дна вертлюжної западини, хоча обидва ці фактори мають аналогічний механізм впливу. І потовщення дна вертлюжної западини, і латералізація центра обертання головки стегнової кістки збільшують плече сили гравітації. Але кути дії сил м’язів-абдукторів при латералізації центра обертання головки стегнової кістки змінюються більшою мірою, і здебільшого зменшуються плечі сил м’язів групи абдукторів стегна. Цим і пояснюється така помітна відмінність у впливі цих факторів на роботу абдукційного механізму кульшового суглоба;
— маса тіла пацієнта має дуже вагомий негативний вплив на роботу абдукційного механізму.
Основні завдання даного дослідження: показати вплив окремих геометричних параметрів кульшового суглоба на функцію м’язів тазового пояса; показати, яким чином і за рахунок чого погіршується робота абдукційного механізму кульшового суглоба при дисплазії; виявити приховані резерви для покращення роботи м’язів — стабілізаторів кульшового суглоба. Проведені нами дослідження продемонстрували, що основні параметри кульшового суглоба, що визначають величину плеча сили абдукторів стегна, доцільно розглядати як біомеханічні критерії ефективності роботи м’язів кульшового суглоба, а біомеханічні рішення в стратегії оперативного лікування коксартрозу відіграють ключову роль у забезпеченні нормальної роботи ендопротеза кульшового суглоба [12].
Особливе значення це має при диспластичному коксартрозі, тому що саме дисплазія кульшового суглоба викликає цілий каскад взаємопов’язаних біомеханічних порушень, що не тільки впливають на геометричні параметри суглоба, але і порушують роботу м’язів.
Ендопротезування кульшового суглоба практично завжди усуває більшість наявних геометричних протиріч між проксимальним відділом стегнової кістки та вертлюжною западиною, а якщо і залишаються якісь залишкові невідповідності, то вони компенсуються під час ходьби завдяки роботі м’язів [13].
Але, на жаль, відновити правильну біомеханіку штучного суглоба не завжди вдається [13], тому що дуже складно врахувати при плануванні та виконанні операції ендопротезування всі сформовані за час хвороби компенсаторні та адаптаційні реакції і стереотипи рухів, які будуть частково зруйновані. Нові ж рухові стратегії повинні бути вироблені з урахуванням нових умов роботи м’язів, що змінилися.
Висновки
1. Розроблена нами математична модель роботи м’язів тазового пояса при дисплазії кульшового суглоба відображає клінічні прояви диспластичного коксартрозу та дозволяє вивчати особливості роботи м’язів тазового пояса до та після ендопротезування диспластичного кульшового суглоба.
2. Зміна геометричних параметрів кульшового суглоба призводить до порушення функції м’язів тазового пояса та зменшує ефективність роботи абдукційного механізму. Найбільш значимий негативний вплив на роботу м’язів тазового пояса справляють геометричні зміни кульшового суглоба, які збільшують момент сили гравітації та зменшують момент сили м’язів-абдукторів (збільшення ШДК стегнової кістки, згинально-привідна контрактура, потовщення дна вертлюжної западини більше 5 мм, латералізація центра обертання головки стегнової кістки та збільшення ваги пацієнта).
3. Корекція зазначених параметрів при ендопротезуванні кульшового суглоба покращує біомеханічні умови роботи м’язів тазового пояса і підвищує ефективність абдукційного механізму.
4. Отримані результати показали, яким чином диспластичні зміни кульшового суглоба негативно впливають на роботу м’язів тазового пояса, та довели, що найважливішими факторами ефективної роботи абдукційного механізму є сила м’язів та вага пацієнта. І саме ці фактори справляють значний вплив на роботу м’язів тазового пояса щодо збереження горизонтальної рівноваги таза.
Конфлікт інтересів. Автори заявляють про відсутність конфлікту інтересів та власної фінансової зацікавленості при підготовці даної статті.
Отримано/Received 06.01.2022
Рецензовано/Revised 17.01.2022
Прийнято до друку/Accepted 20.01.2022
Список литературы
1. Flecher X. Evaluation of the hip center in total hip arthroplasty for old developmental dysplasia. J. Arthroplasty. 2008. Vol. 23. № 8. P. 1189-1196. DOI: 10.1016/j.arth.2007.10.008.
2. Ganz R., Leunig M. Morphological variations of residual hip dysplasia in the adult. Hip Int. 2008. Vol. 17. Suppl. 5. P. 22-28. Doi: 10.1177/112070000701705S04.
3. Emrah Kovalak, Hanife Özdemir, Cenk Ermutlu, Abdullah Obut. Assessment of hip abductors by MRI after total hip arthroplasty and effect of fatty atrophy on functional outcome. Acta Orthop. Traumatol. Turc. 2018 May. 52(3). Р. 196-200. doi: 10.1016/j.aott.2017.10.005.
4. Yang S., Cui Q. Total hip arthroplasty in developmental dysplasia of the hip: Review of anatomy, techniques and outcomes. World J. Orthop. 2012. Vol. 3. № 5. P. 42-48. DOI: 10.5312/wjo.v3.i5.42.
5. Meyer C.A.G., Wesseling M., Corten K., Nieuwenhuys A., Monari D., Simon J.-P., Jonkers I., Desloovere K. Hip movement pathomechanics of patients with hip osteoarthritis aim at reducing hip joint loading on the osteoarthritic side. Gait Posture. 2018 Jan. 59. Р. 11-17. doi: 10.1016/j.gaitpost.2017.09.020.
6. Levin S., de Solórzano S.L., Scarr G. The significance of closed kinematic chains to biological movement and dynamic stability. J. Bodyw. Mov. Ther. 2017. Vol. 21. № 3. P. 664-672. DOI: 10.1016/j.jbmt.2017.03.012.
7. Тяжелов А., Карпинский М.Ю., Карпинская Е.Д., Гончарова Л.Д., Климовицкий Р.В. Моделирование работы мышц тазового пояса после эндопротезирования тазобедренного сустава при различной величине общего бедренного офсета. Травма. 2017. Т. 18. № 6. С. 133-141. DOI: 10.22141/1608-1706.6.18.2017.121191.
8. Crowe J.F., Mani V.J., Ranawat S. Total hip replacement in congenital dislocation and dysplasia of the hip. J. Bone Joint Surg. Am. 1979. 61(1). Р. 15-23. PMID: 365863.
9. Carhart M.R. Biomechanical Analysis of Compensatory Stepping: Implications for Paraplegics Standing Via FNS, PhD. Dissertation, Arizona State University, 2000.
10. Тяжелов А.А., Карпинская Е.Д., Гончарова Л.Д., Климовицкий Ф.В. Особенности работы абдукционного механизма до и после тотального эндопротезирования тазобедренного сустава. Мир медицины и биологии. 2020. № 3(73). С. 134-139. DOI: 10.26724/2079-8334-2020-3-73-134-139.
11. Ong K.L., Manley M.T., Nevelos J., Greene K. Review: biomechanical issues in total hip replacement. Surg. Technol. Int. 2012. Dec. 22. Р. 222-8. PMID: 23023572.
12. Takabayashi I.T., Kubo E.M. Evaluation of factors that affect hip moment impulse during gait: A systematic review. Gait Posture. 2018 Mar. 61. Р. 488-492. doi: 10.1016/j.gaitpost.2018.02.017.
13. Tsai T., Dimitriou D., Li G., Kwon Y. Does total hip arthroplasty restore native hip anatomy? Three-dimensional reconstruction analysis. International Orthopaedics. 2014. 38(8). Р. 1577-1583. doi: 10.1007/s00264-014-2401-3.

/5.jpg)
/6.jpg)
/6_2.jpg)
/6_3.jpg)
/6_4.jpg)
/6_5.jpg)
/6_6.jpg)
/6_7.jpg)
/7.jpg)
/8.jpg)
/8_2.jpg)
/9.jpg)