
Журнал «Травма» Том 24, №4, 2023
Вернуться к номеру
Доцільність використання оціночних шкал H. Kitaoka (AOFAS), FFI (Italian version), Roles і Maudsley, VAS у пацієнтів із плоскою стопою
Авторы: Лябах А.П., Турчин О.А., Пятковський В.М.
ДУ «Інститут травматології та ортопедії НАМН України», м. Київ, Україна
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
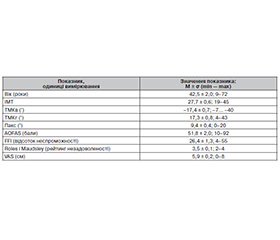
Оцінка функціональної спроможності стопи потребує адекватних інструментів залежно від конкретної нозології. Мета: дослідити можливість застосування оціночних шкал H. Kitaoka (American Orthopaedic Foot and Ankle Society (AOFAS)), Foot Function Index (FFI) (Italian version), Roles і Maudsley, візуальної аналогової шкали (VAS) у пацієнтів із плоскою стопою (ПС). Матеріали та методи. Проведено клінічне й рентгенологічне дослідження 63 пацієнтів (78 стоп), які мали ПС. Вік пацієнтів становив у середньому 42,5 ± 2,0 року (9–72 роки). Були використані скіалогічні й клінічні показники: горизонтальний і вертикальний талометатарзальний кути, кут вальгусного відхилення п’яткової кістки, індекс маси тіла. Оцінку функціонального стану стопи проводили за шкалами H. Kitaoka (AOFAS), FFI (Italian version), Roles і Maudsley, VAS. Силу зв’язку між показниками вивчали за допомогою парних кореляцій Пірсона, кореляційно-регресійний аналіз проводили на моделях, у яких залежними змінними виступали показники оціночних шкал. Результати. Встановлена обернена залежність бальної оцінки функції стопи (AOFAS) від віку і значень вертикального талометатарзального кута, пряма залежність індексу неспроможності стопи (FFI) від віку та індексу маси тіла, пряма залежність функціональної недостатності (Roles і Maudsley) і рівня болю (VAS) від віку. Встановлено достатній ступінь кореляції (0,5–0,75) між застосованими шкалами. Висновки. Встановлена достатня критеріальна і конструктна валідність шкал AOFAS, FFI (Italian version), Roles і Maudsley, VAS при застосуванні в пацієнтів із ПС. Застосування обраних шкал є адекватним інструментом для оцінки функціональної спроможності пацієнтів із ПС.
Assessment of the functional capacity of the foot requires adequate tools depending on a specific nosology. Objective: to investigate the possibility of using evaluation scale of H. Kitaoka (American Orthopaedic Foot and Ankle Society (AOFAS)), Foot Function Index (FFI) (Italian version), Roles and Maudsley score, visual analog scale (VAS) in patients with flatfoot. Materials and methods. Clinical and X-ray examinations of 63 patients (78 feet) who had flatfoot were performed. Their average age was 42.5 ± 2.0 (9–72) years. X-ray and clinical indicators were used: horizontal and vertical talo-metatarsal angles (TMA), angle of valgus deviation of the calcaneus, body mass index. The assessment of the functional state of the foot was carried out according to the H. Kitaoka (AOFAS) scale, FFI (Italian version), Roles and Maudsley score, VAS. The strength of the relationship between indicators was studied using Pearson’s pairwise correlations; a correlation regression analysis was performed on models where the indicators of rating scales were the dependent variables. Results. There was an inverse correlation between the foot function score (AOFAS) and the age and TMA, a direct correlation between the FFI and the age and body mass index, a direct dependence of functional insufficiency (Roles and Maudsley score) and pain level (VAS) on age. A sufficient degree of correlation (0.5–0.75) was found between the applied scales. Conclusions. Sufficient criterial and construct validity of the AOFAS scale, FFI (Italian version), Roles and Maudsley score, VAS was found when used in patients with flatfoot. The use of selected scales is an adequate tool for assessing functional capacity in patients with flatfoot.
плоска стопа; PROMs; шкала AOFAS; Foot Function Index (Italian version); шкала Roles і Maudsley; візуальна аналогова шкала
flat foot; patient-reported outcome measures; American Orthopaedic Foot and Ankle Society scale; Foot Function Index (Italian version); Roles and Maudsley score; visual analog scale