
Международный эндокринологический журнал Том 20, №4, 2024
Вернуться к номеру
Підвищення альбумін-креатинінового співвідношення сечі як один з найбільш ранніх маркерів ураження нирок у хворих на артеріальну гіпертензію та цукровий діабет 2-го типу
Авторы: Коваль С.М., Рєзнік Л.А., Старченко Т.Г., Милославський Д.К.
ДУ «Національний інститут терапії імені Л.Т. Малої НАМН України», м. Харків, Україна
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
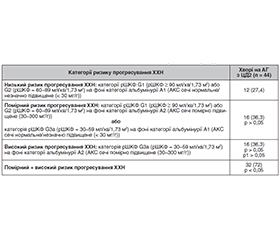
Актуальність. Поєднаний перебіг артеріальної гіпертензії (АГ) та цукрового діабету 2-го типу (ЦД2) асоціюється з особливо високим ризиком серцево-судинних і ниркових ускладнень. Відповідно до чинних міжнародних рекомендацій для діагностики хронічної хвороби нирок (ХХН) використовують два критерії: розрахункова швидкість клубочкової фільтрації (рШКФ) та альбумін-креатинінове співвідношення (АКС) сечі. Але на сьогодні характер і етапність змін АКС сечі та їх взаємозв’язок зі змінами рШКФ у хворих на АГ з ЦД2 недостатньо вивчені. Мета: вивчення частоти і вираженості підвищення АКС сечі у хворих на АГ з ЦД2. Матеріали та методи. Обстежено 44 хворі на АГ ІІ стадії, 2–3-го ступеня з ЦД2 віком від 40 до 64 років: чоловіків — 20 (45 %), жінок — 24 (55 %). Обстеження хворих проводили з використанням стандартних клінічних, антропометричних, лабораторних та інструментальних методів. Діагностику АГ, ЦД2, серцево-судинних захворювань, їх факторів ризику, ХХН та категорій змін рШКФ і альбумінурії оцінювали згідно з європейськими та українськими рекомендаціями. Визначення рШКФ проводили за формулою CKD-EPI з урахуванням рівнів креатиніну сироватки крові, альбумінурію діагностували за допомогою оцінки АКС у ранковій порції сечі. Результати. При аналізі змін рШКФ у 41 % хворих на АГ з ЦД2 реєструється зниження рШКФ до категорії G3a, що вказує на наявність ураження нирок як органа-мішені. Аналіз змін АКС сечі дозволяє виявити ураження нирок як органа-мішені (помірне підвищення АКС сечі до категорії А2) у вірогідно більшої частини хворих — у 65 % осіб. Помірне підвищення АКС у сечі діагностується не тільки у переважної більшості хворих на АГ з ЦД2 зі зниженням рШКФ до категорії G3a (у 89 % осіб), але й у 55 % хворих з незначним зниженням рШКФ (категорія G2), а також у 25 % хворих з нормальним або високим показником рШКФ. Визначення ризику прогресування ХХН на підставі одночасного аналізу показника рШКФ і показника АКС в сечі свідчить про те, що у переважної більшості хворих на АГ з ЦД2 (72 %) існує підвищений ризик прогресування ХХН, і тільки менше ніж третина таких хворих може бути віднесена до категорії низького ризику прогресування ХХН. Висновки. Підвищення показника АКС сечі може розглядатись як більш ранній маркер ураження нирок у хворих на АГ з ЦД2, ніж зниження рШКФ, яке визначається за рівнем креатиніну в сироватці крові. Визначення АКС сечі повинно проводитись додатково до визначення рШКФ у всіх хворих цієї категорії з метою найбільш ранньої діагностики ураження нирок та прогнозування ризику прогресування ХХН і серцево-судинних ускладнень.
Background. The combination of hypertension and type 2 diabetes mellitus (T2DM) is associated with a particularly high risk of cardiovascular and renal complications. In accordance with current international guidelines, two criteria are used to diagnose chronic kidney disease (CKD): estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (ACR). However, at present, the nature and stages of changes in urine ACR and their relationship with changes in eGFR in hypertensive patients with T2DM have not been sufficiently studied. The purpose was to investigate the frequency and severity of increased urine ACR in hypertensive patients with T2DM. Materials and methods. We examined 44 patients with stage II hypertension grade 2–3 and T2DM aged 40 to 64 years: 20 (45 %) men, 24 (55 %) women. The examination was carried out using standard clinical, anthropometric, laboratory and instrumental methods. Diagnosis of hypertension, T2DM, cardiovascular diseases, their risk factors, CKD and categories of changes in eGFR and albuminuria were assessed in accordance with European and Ukrainian guidelines. eGFR was calculated using the CKD-EPI equation, taking into account serum creatinine levels; albuminuria was diagnosed by assessing ACR in the morning urine. Results. When analyzing changes in eGFR, 41 % of hypertensive patients with T2DM had a decrease in eGFR to G3a category, which indicates the presence of kidney damage as a target organ. Analysis of changes in urine ACR allows us to identify kidney damage as a target organ (a moderate increase in urine ACR to A2 category) in a significantly larger proportion of patients — 65 % of people. A moderate increase in urine ACR is diagnosed not only in most hypertensive patients with T2DM with a decrease in eGFR to G3a category (89 % of cases), but also in 55 % of individuals with a slight decrease in eGFR (G2 category), as well as in 25 % of patients with normal or high eGFR. Determining the risk of CKD progression based on simultaneous analysis of eGFR and urine ACR indicates that the vast majority of hypertensive patients with T2DM (72 %) have an increased risk of CKD progression, and only less than a third can be classified as those at risk of CKD progression. Conclusions. An increase in urine ACR can be considered as an earlier marker of kidney damage in hypertensive patients with T2DM than a decrease in eGFR, determined by the level of creatinine in the blood serum. Evaluation of urine ACR should be carried out in addition to the determination of eGFR in all patients in this category in order to diagnose kidney damage as early as possible and predict the risk of CKD progression and cardiovascular complications.
артеріальна гіпертензія; цукровий діабет 2-го типу; хронічна хвороба нирок; розрахункова швидкість клубочкової фільтрації; альбумін-креатинінове співвідношення сечі
hypertension; type 2 diabetes mellitus; chronic kidney disease; estimated glomerular filtration rate; urine albumin-to-creatinine ratio
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Mancia G, Kreutz R, Brunström M. et al. 2023 ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens. 2023 Dec 1;41(12):1874-2071. doi: 10.1097/HJH.0000000000003480. Epub 2023 Sep 26. Erratum in: J Hypertens. 2024 Jan 1;42(1):194. PMID: 37345492.
- Koval S, Penkova M, Mysnychenko O. Changes in the nature of the disease in patients with hypertension and type 2 diabetes mellitus — representatives of the civilian population after a long stay in the combat zone. International Journal оf Endocrinology (Ukraine). 2023;19(8):586-591. https://doi.org/10.22141/2224-0721.19.8.2023.1342.
- Pankiv V. Type 2 diabetes mellitus: current international guidelines, personalized approach and real outpatient practice. International Journal оf Endocrinology (Ukraine). 2020;16(6):463-470. https://doi.org/10.22141/2224-0721.16.6.2020.215384.
- Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, et al. IDF Diabetes Atlas: Global, regional and country-le–vel diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022 Jan;183:109119. doi: 10.1016/j.diabres.2021.109119. Epub 2021 Dec 6. Erratum in: Diabetes Res Clin Pract. 2023 Oct;204:110945. PMID: 34879977; PMCID: PMC11057359.
- Marx N, Federici M, Schütt K, Müller-Wieland D, et al. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes: Developed by the task force on the management of cardiovascular disease in patients with diabetes of the European Society of Cardiology (ESC). European Heart Journal. 2023;44, Iss 39:4043-4140. https://doi.org/10.1093/eurheartj/ehad192.
- Tuttolomondo A, Cirrincione A, Casuccio A, et al. Efficacy of dulaglutide on vascular health indexes in subjects with type 2 diabetes: a randomized trial. Cardiovasc Diabetol. 2021 Jan 4;20(1):1. doi: 10.1186/s12933-020-01183-5. PMID: 33397395; PMCID: PMC7784355.
- Koval SM, Yushko KO. Type 2 diabetes mellitus and cardiovascular disease. Part I. Definition of the problem, stratification of cardiovascular risk and the main directions of prevention of cardiovascular diseases in patients with type 2 diabetes mellitus. Hypertension;13(5):11-19. https://doi.org/10.22141/2224-1485.13.5.2020.218437.
- Wlodarczyk B, Borkowska A, Wlodarczyk P, Malecka-–Panas E, Gasiorowska A. Serum Levels of Insulin-like Growth Factor 1 and Insulin-like Growth Factor-binding Protein 2 as a Novel Biomar–ker in the Detection of Pancreatic Adenocarcinoma. J Clin Gastroente–rol. 2020 Oct;54(9):e83-e88. doi: 10.1097/MCG.0000000000001297. PMID: 31851103.
- Liu J, Zhuang T, Pi J, Chen X, Zhang Q, Li Y, et al. Endothelial Forkhead Box Transcription Factor P1 Regulates Pathological Cardiac Remodeling Through Transforming Growth Factor-β1-Endothelin-1 Signal Pathway. Circulation. 2019 Aug 20;140(8):665-680. doi: 10.1161/CIRCULATIONAHA.119.039767. Epub 2019 Jun 10. PMID: 31177814.
- Yao ZH, Xie HJ, Yuan YL, Huo YT, Cao J, Lai WY, et al. Contraction-dependent TGF-β1 activation is required for thrombin-induced remodeling in human airway smooth muscle cells. Life Sci. 2018 Mar 15;197:130-139. doi: 10.1016/j.lfs.2018.02.012. Epub 2018 Feb 8. PMID: 29428600.
- Chernyshov VA, Nesen AO, Semenovyh PS, Shkapo VL. Risk Factors Associated with Diabetic Nephropathy and Their Clinical Significance. Ukrainian Journal of Medicine, Biology and Sports. 2022;7(39):57-64. DOI: 10.26693/jmbs07.05.057.
- Kidney Disease: Improving Global Outcomes (KDIGO) Dia–betes Work Group. KDIGO 2022 Clinical Practice Guideline for Dia–betes Management in Chronic Kidney Disease. Kidney Int. 2022 Nov;102(5S):S1-S127. doi: 10.1016/j.kint.2022.06.008. PMID: 36272764.
- Abdelwahid HA, Dahlan HM, Mojemamy GM, Darraj GH. Predictors of microalbuminuria and its relationship with glycemic control among Type 2 diabetic patients of Jazan Armed Forces Hospital, southwestern Saudi Arabia. BMC Endocrine Disorders. 2022;22:307. https://doi.org/10.1186/s12902-022-01232-y.
- Summary of Recommendation Statements. Kidney Int Suppl (2011). 2013 Jan;3(1):5-14. doi: 10.1038/kisup.2012.77. PMID: 25598998; PMCID: PMC4284512.
- Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al.; CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009 May 5;150(9):604-12. doi: 10.7326/0003-4819-150-9-200905050-00006. Erratum in: Ann Intern Med. 2011 Sep 20;155(6):408. PMID: 19414839; PMCID: PMC2763564.
- Matsushita K, Mahmoodi BK, Woodward M, Emberson JR, Jafar TH, Jee SH, et al.; Chronic Kidney Disease Prognosis Consortium. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA. 2012 May 9;307(18):1941-51. doi: 10.1001/jama.2012.3954. PMID: 22570462; PMCID: PMC3837430.
- Cardiovascular diseases. Classification, standards of diagnosis and treatment. Еdited by V.M. Kovalenko, M.I. Lutaya, Sirenko Y.M., Sychova O.S. K.: MORION, 2021. 320.
- Unified clinical protocol of primary and secondary (speciali–zed) medical care. Type 2 diabetes. Order of the Ministry of Health of Ukraine. 12/21/2012, No. 1118:115. URL: https://ips.ligazakon.net/document/view/moz21173.
- Diabetes. Evidence-based Clinical guideline, Ministry of Health of Ukraine. 2022:347. https://moz.gov.ua/uploads/ckeditor/.
- Boenink R, Astley ME, Huijben JA, Stel VS, Kerschbaum J, Ots-Rosenberg M, et al. The ERA Registry Annual Report 2019: summary and age comparisons. Clin Kidney J. 2022;15:452-472.
- Kosiborod MN, Bhatta M, Davies M, Deanfield JE, Garvey WT, Khalid U, et al. Semaglutide improves cardiometabolic risk factors in adults with overweight or obesity: STEP 1 and 4 explora–tory analyses. Diabetes Obes Metab. 2023 Feb;25(2):468-478. doi: 10.1111/dom.14890. Epub 2022 Oct 28. PMID: 36200477; PMCID: PMC10092593.
- Ali A, Taj A, Amin MJ, Iqbal F, Iqbal Z. Correlation between Microalbuminuria and Hypertension in Type 2 Diabetic Patients. Pak J Med Sci. 2014 May;30(3):511-4. doi: 10.12669/pjms.303.5042. PMID: 24948969; PMCID: PMC4048496.
- Bae ES, Hur JY, Jang HS, Kim JS, Kang HS. Risk Factors of Microalbuminuria among Patients with Type 2 Diabetes Mellitus in Korea: A Cross-Sectional Study Based on 2019-2020 Korea National Health and Nutrition Examination Survey Data. Int J Environ Res Public Health. 2023 Feb 25;20(5):4169. doi: 10.3390/ijerph20054169. PMID: 36901179; PMCID: PMC10002237.
- Matsushita K, van der Velde M, Astor BC et al. Chronic Kidney Disease Prognosis Consortium Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010 Jun 12;375(9731):2073-81. doi: 10.1016/S0140-6736(10)60674-5. Epub 2010 May 17. PMID: 20483451; PMCID: PMC3993088.
- Fox CS, Matsushita K, Woodward M, et al. Chronic Kidney Disease Prognosis Consortium. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and wit–hout diabetes: a meta-analysis. Lancet. 2012 Nov 10;380(9854):1662-73. doi: 10.1016/S0140-6736(12)61350-6. Epub 2012 Sep 24. Erratum in: Lancet. 2013 Feb 2;381(9864):374. PMID: 23013602; PMCID: PMC3771350.
- Zeng C, Zhang Y, Deng S, Xin Y, Hu X. Association of Urine Albumin to Creatinine Ratio with Cardiovascular Outcomes in Patients with Type 2 Diabetes Mellitus. The Journal of Clinical Endocrinology & Metabolism. 2023;1-14. https://doi.org/10.1210/clinem/dgad645.
- McGill JB, Haller H, Roy-Chaudhury P, Cherrington A, Wada T, Wanner C, et al. Making an impact on kidney disease in people with type 2 diabetes: The importance of screening for albumi–nuria BMJ Open Diabetes Res Care. 2022 Jul;10(4): e 002806. doi: 10.1136/bmjdrc-2022-002806. PMID: 35790319.