
Журнал «Медицина неотложных состояний» Том 20, №8, 2024
Вернуться к номеру
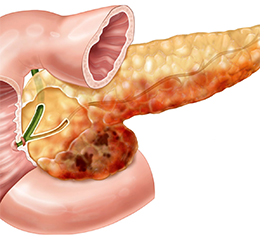
Досвід оперативного лікування бойової травми підшлункової залози
Авторы: E.M. Khoroshun (1, 2), I.P. Khomenko (3, 4), S.A. Shipilov (1, 2), V.V. Makarov (1, 2), V.V. Nehoduiko (1, 2), O.H. Petiunin (1, 5)
(1) - Kharkiv National Medical University, Kharkiv, Ukraine
(2) - Military Medical Clinical Center of the Northern Region, Kharkiv, Ukraine
(3) - National Academy of Medical Sciences of Ukraine, Kyiv, Ukraine
(4) - Kyiv City Clinical Hospital 8, Kyiv, Ukraine
(5) - Kharkiv Institute of Medicine and Biomedical Sciences, Kharkiv, Ukraine
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
Актуальність. Поранення підшлункової залози, особливо бойові, є складним завданням для хірургів-травматологів через наявність поєднаних ушкоджень та ускладнень. Мета: надати структуру, особливості діагностики й лікування бойової травми підшлункової залози. Матеріали та методи. Проведено ретроспективний аналіз медичних карт 58 пацієнтів, які отримали бойову травму підшлункової залози під час війни в Україні. Їхній середній вік становив 37,4 ± 3,6 року (діапазон 21–60 років). Механізм бойової травми: вогнепальні поранення — 87,9 %, вибухові — 10,3 %, закриті травми — 1,7 %. Усім хворим виконували лабораторні й інструментальні дослідження. Результати. За характером бойової травми розподіл ушкоджень підшлункової залози наступний: вогнепальні осколкові — 50 (86,2 %), вогнепальні кульові — 1 (1,7 %), вибухові — 6 (10,3 %), закриті — 1 (1,7 %). Розподіл за локалізацією ушкодження підшлункової залози: хвіст — 38 (65,5 %), голівка — 11 (19 %), тіло — 5 (8,6 %), тіло й хвіст — 2 (3,4 %), голівка та хвіст — 2 (3,4 %). Проведені оперативні втручання: за методикою DCS — 51 (87,9 %), одноетапна операція — 7 (12,1 %). Розподіл за видом оперативного втручання: дренування парапанкреатичного простору — 45 (77,6 %), панкреаторафія — 4 (6,9 %), дистальна панкреатоспленектомія — 3 (5,2 %), видалення сторонніх тіл (металевих осколків) — 3 (5,2 %), дистальна резекція підшлункової залози зі збереженням селезінки — 1 (1,7 %), панкреатодуоденектомія — 1 (1,7 %), субтотальна резекція тіла й хвоста підшлункової залози зі спленектомією — 1 (1,7 %). Загальні ускладнення (n = 42): перитоніт — 9 (21,4 %), гострий хірургічний сепсис — 8 (19 %), гостра ниркова недостатність — 7 (16,7 %), синдром поліорганної недостатності — 7 (16,7 %), пневмонія — 6 (14,3 %), кровотеча — 4 (9,5 %), тромбоемболія легеневої артерії — 1 (2,4 %). Органоспецифічні ускладнення (n = 28): гострий панкреатит — 21 (75 %), панкреатичні нориці — 4 (14,3 %), псевдокісти — 2 (7,1 %), абсцес — 1 (3,6 %) випадок. Результати лікування: переведені на наступний етап лікування — 33 (56,9 %), померли — 19 (32,8 %), виписані з визначеним результатом — 6 (10,3 %) пацієнтів. За летальністю: померли в перші 3 доби — 5 (26,3 %), у період від 4 до 15 діб — 14 (73,7 %) осіб. Висновки. Частота бойового ушкодження підшлункової залози серед абдомінальних травм становить 8,7 %. Хірургічне лікування бойової травми підшлункової залози за методикою DCS проводиться у 87,9 % випадків, а в обсязі одноетапної операції — у 12,1 %. Використання методики DCS приводить до зниження частоти ускладнень. Загальна частота ускладнень становить 72,4 %, органоспецифічних — 48,3 %. Летальність зафіксовано в 32,8 % випадків. Бойову травму голівки підшлункової залози лікували переважно за допомогою закритого дренування, дистальні травми — резекції або дренування.
Background. Pancreatic injuries is a complex challenge for trauma surgeons, especially if combat, due to the presence of combined injuries and complications. The aim: to provide a structure, peculiarities of diagnosis and treatment of combat pancreatic trauma. Materials and methods. A retrospective analysis was done of medical records of 58 inpatients who sustained combat pancreatic trauma during the war in Ukraine. Their average age was 37.4 ± 3.6 years (range 21–60 years). The mechanism of combat injury included gunshot wounds (87.9 %), explosive (10.3 %) and closed injuries (1.7 %). All the wounded underwent laboratory and instrumental investigations. Results. According to the nature of the combat injury, pancreatic injuries were categorised into gunshot shrapnel wounds — 50 (86.2 %), gunshot bullet wounds — 1 (1.7 %), explosive trauma — 6 (10.3 %), and closed combat trauma — 1 (1.7 %) case. Distribution by location of pancreatic injury: tail — 38 (65.5 %), head — 11 (19 %), body — 5 (8.6 %), body and tail — 2 (3.4 %), head and tail — 2 (3.4 %) cases. The following methods of surgical intervention were used: damage control surgery (DCS) — 51 (87.9 %) cases, one-stage surgery — 7 (12.1 %) cases. Distribution by the type of surgical intervention for pancreatic injury: drainage of the parapancreatic space — 45 (77.6 %), pancreatorrhaphy — 4 (6.9 %), distal pancreatosplenectomy — 3 (5.2 %), removal of foreign bodies (metal fragments) — 3 (5.2 %), distal resection of the pancreas with spleen preservation — 1 (1.7 %), pancreatoduodenectomy — 1 (1.7 %), subtotal resection of the body and tail of the pancreas with splenectomy — 1 (1.7 %) case. Common complications (n = 42): peritonitis — 9 (21.4 %), acute surgical sepsis — 8 (19 %), acute renal failure — 7 (16.7 %), multiple organ failure syndrome — 7 (16.7 %), pneumonia — 6 (14.3 %), bleeding — 4 (9.5 %), pulmonary embolism — 1 (2.4 %). Organ-specific complications (n = 28) were as follows: acute pancreatitis — 21 (75 %), pancreatic fistula — 4 (14.3 %), pseudocysts — 2 (7.1 %), abscess — 1 (3.6 %) case. Treatment outcomes: 33 patients (56.9 %) were transferred to the next stage of treatment, 19 (32.8 %) died, and 6 (10.3 %) were discharged with a definite outcome. Mortality rate: 5 (26.3 %) died in the first 3 days, 14 (73.7 %) cases died in the period from 4 to 15 days. Conclusions. The incidence of combat pancreatic trauma among abdominal wounds is 8.7 %. Surgical treatment for combat pancreatic trauma using the DCS is performed in 87.9 % of cases, and in the volume of a single-stage operation, in 12.1 %. The DCS leads to a reduction in the incidence of complications. The overall complication rate for combat pancreatic trauma is 72.4 %, and the incidence of organ-specific complications is 48.3 %. Mortality from pancreatic injuries is 32.8 %. Combat trauma to the head of the pancreas was mainly treated with closed drainage. Distal injuries were treated by resection or drainage.
ушкодження підшлункової залози; вогнепальні поранення; бойові травми; оперативне лікування
pancreatic injury; gunshot wounds; combat trauma; surgical treatment
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Атлас бойової хірургічної травми (досвід антитерористичної операції/операції об’єднаних сил). Під заг. ред. В.І. Цимбалюка. Харків: Колегіум, 2021. 385 с.
- Гречаник О.І., Абдуллаєв Р.Я., Лурін І.А., Гуменюк К.В., Негодуйко В.В., Слесаренко Д.О. Сучасні аспекти діагностики вогнепальних поранень живота. Досвід гібридної війни на сході України. Клінічна хірургія. 2021;88(5–6):42-52. doi: 10.26779/2522-1396.2021.5-6.42.
- Лікування поранених з бойовими ушкодженнями живота (за досвідом АТО/ООС): монографія / За ред. К.В. Гуменюка, І.П. Хоменка, І.А. Луріна та ін.; за заг. ред. В.І. Цимбалюка. Херсон: Олді+, 2022. 194 с.
- Agarwal H, Gupta A, Kumar S. An overview of Pancreatic Trauma. J Pancreatol. 2020;3:139-146. doi: 10.1097/JP9.0000000000000044.
- Niwano F, Babaya N, Hiromine Y, Matsumoto I, Kamei K, et al. Glucose Metabolism After Pancreatectomy: Opposite Extremes Between Pancreaticoduodenectomy and Distal Pancreatectomy. J Clin Endocrinol Metab. 2021 Apr 23;106(5):e2203-e2214. doi: 10.1210/clinem/dgab036.
- Alzerwi NAN. Injury characteristics and predictors of mortality in patients undergoing pancreatic excision after abdominal trauma: A National Trauma Data Bank (NTDB) study. Medicine (Baltimore). 2023 Jun 16;102(24):e33916. doi: 10.1097/MD.0000000000033916.
- Tuşat M, Özmen İ, Demirtaş MS, Ateş C, Öztürk AB, Kankılıç NA, Başar D. Risk factors for mortality and morbidity in Syrian refugee children with penetrating abdominal firearm injuries: an 1-year experience. Ulus Travma Acil Cerrahi Derg. 2023 Sep;29(9):1051-1060. doi: 10.14744/tjtes.2023.70658.
- Belhadj A, Saidani A, Touati MD, et al. Case series: Mana-
- gement and outcomes of five cases of blunt and open pancreatic trauma. F1000Research. 2024;13:573. doi: 10.12688/f1000research.152067.1.
- Kuza CM, Hirji SA, Englum BR, Ganapathi AM, Speicher PJ, Scarborough JE. Pancreatic Injuries in Abdominal Trauma in US Adults: Analysis of the National Trauma Data Bank on Management, Outcomes, and Predictors of Mortality. Scandinavian Journal of Surgery. 2020;109(3):193-204. doi: 10.1177/1457496919851608.
- Menahem B, Lim C, Lahat E, Salloum C, Osseis M, Lacaze L, et al. Conservative and surgical management of pancreatic trauma in adult patients. Hepatobiliary Surg Nutr. 2016;5:470-477. doi: 10.21037/hbsn.2016.07.01.
- Addison P, Iurcotta T, Amodu LI, Crandall G, Akerman M, Galvin D, et al. Outcomes following operative vs. non-operative ma-nagement of blunt traumatic pancreatic injuries: a retrospective multi-institutional study. Burn Trauma. 2016;4:39. doi: 10.1186/s41038-016-0065-5.
- Farrell RJ, Krige JE, Bornman PC, Knottenbelt JD, Terblanche J. Operative strategies in pancreatic trauma. Br J Surg. 1996;83:934-937.
- Arvieux C, Guillon F, Létoublon Ch, Oughriss M. Pancreatic trauma. J Chir (Paris). 2003 Oct;140(5):261-9 (in French).
- Cinquantini F, Tugnoli G, Piccinini A, Coniglio C, Mannone S, Biscardi A, et al. Educational review of predictive value and findings of computed tomography scan in diagnosing bowel and me-senteric injuries after blunt trauma: correlation with trauma surgery findings in 163 patients. Can Assoc Radiol J. 2017;68:276-285. doi: 10.1016/j.carj.2016.07.003.
- Gong SC, An S, Shin IS, Jung PY. Usefulness of Endoscopic Retrograde Cholangiopancreatography in the Diagnosis and Treatment of Traumatic Pancreatic Injury in Children. Diagnostics. 2023;13(12):2044. doi: 10.3390/diagnostics13122044.
- 16. Zantut LF, Ivatury RR, Smith RS, Kawahara NT, Porter JM, Fry WR, et al. Diagnostic and therapeutic laparoscopy for penetrating abdominal trauma: a multicenter experience. J Trauma. 1997;42:825-829. doi: 10.1097/00005373-199705000-00012.
- Coccolini F, Kobayashi L, Kluger Y, Moore EE, Ansaloni L, et al.; WSES-AAST Expert Panel. Duodeno-pancreatic and extrahepatic biliary tree trauma: WSES-AAST guidelines. World J Emerg Surg. 2019 Dec 11;14:56. doi: 10.1186/s13017-019-0278-6.
- Haroon HM, Aljoufi A, Khudhayr E, Shamshad H. Penetra-ting Abdominal Injuries in War Victims Challenges and Management Controversies. Genesis J Surg Med. 2023;2(2):1-8.
- Hecker A, Hecker M, Riedel JG, Hecker B, Doppstadt C, et al. New WSES-AAST guideline on duodeno-pancreatic and extrahepatic biliary tree trauma: summary and comments. Chirurg. 2020 Aug;91(8):681-684 (in German). doi: 10.1007/s00104-020-01236-1.
- Kanlerd Amonpon, Auksornchart Karikarn, Boonyasatid Piyapong. Non-operative management for abdominal solid organ injuries: A literature review. Chinese Journal of Traumatology. 2022;25(5):249-256. doi: 10.1016/j.cjtee.2021.09.006.
- Lin B-C, Chen R-J, Fang J-F, Hsu Y-P, Kao Y-C, Kao J-L. Management of blunt major pancreatic injury. J Trauma. 2004;56:774-778. doi: 10.1097/01.TA.0000087644.90727.DF.
- De Carvalho Maria Eduarda, Alonso Joaquim, et al. Pancreaticodudonectomy in trauma: One or two stages? Injury. 2020;51(3):592-596. doi: 10.1016/j.injury.2020.01.018.
- Seamon MJ, Kim PK, Stawicki SP, Dabrowski GP, Goldberg AJ, Reilly PM, et al. Pancreatic injury in damage control laparotomies: Is pancreatic resection safe during the initial laparotomy? Injury. 2009;40:61-65. doi: 10.1016/j.injury.2008.08.010.
- Ordoñez C, García A, Parra MW, Scavo D, Pino LF, Millán M, et al. Complex penetrating duodenal injuries: less is better. J Trauma Acute Care Surg. 2014;76:1177-1183. doi: 10.1097/TA.0000000000000214.
- Krige JEJ, Kotze UK, Setshedi M, Nicol AJ, Navsaria PH. Prognostic factors, morbidity and mortality in pancreatic trauma: a critical appraisal of 432 consecutive patients treated at a Level 1 Trauma Centre. Injury. 2015;46:830-836. doi: 10.1016/j.injury.2015.01.032.
- Vengail S, Ajmeera R, Jha RK, Sethi AK, Francis M, Syed AK. Evaluation of the Blunt Pancreatic Injury, a Long-Term Tertiary Care Center Study: An Original Research. J Pharm Bioallied Sci. 2023 Jul;15(Suppl 1):S277-S280. doi: 10.4103/jpbs.jpbs_494_22.
- Krige JE, Beningfield SJ, Nicol AJ, Navsaria P. The management of complex pancreatic injuries. S Afr J Surg. 2005;43:92-102.
- Kumar A, Panda A, Gamanagatti S. Blunt pancreatic trauma: a persistent diagnostic conundrum? World J Radiol. 2016;8:159-173. doi: 10.4329/wjr.v8.i2.159.
- Vertrees A, Elster E, Jindal R, Ricordi C, Shriver C. Surgical management of modern combat-related pancreatic injuries: traditional management and unique strategies. Mil Med. 2014;179:315-319. doi: 10.7205/MILMED-D-13-00375.