
Журнал «Почки» Том 14, №1, 2025
Вернуться к номеру
Аналіз залежності рівнів маркерів раннього ураження нирок — цитокінів КІМ-1 та TGF-β1 у дітей, хворих на ювенільний ідіопатичний артрит
Авторы: L.I. Vakulenko, S.V. Samsonenko
Dnipro State Medical University, Dnipro, Ukraine
Рубрики: Нефрология
Разделы: Клинические исследования
Версия для печати
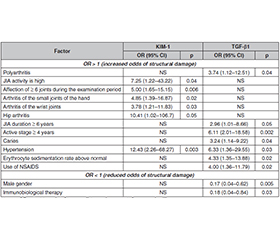
Актуальність. Ювенільний ідіопатичний артрит (ЮІА) є гетерогенною групою захворювань, що характеризуються хронічним запаленням суглобів у дітей віком до 16 років. Ураження нирок при ЮІА варіюють від безсимптомної протеїнурії до тяжкого гломерулонефриту, здатного призвести до хронічної хвороби нирок. З огляду на наведені дані припущення про підвищений ризик раннього ураження нирок у дітей iз ЮІА є обґрунтованим. Мета роботи: проаналізувати фактори ризику розвитку структурних тубулярних уражень шляхом вивчення рівня молекули ушкодження нирок-1 (КІМ-1) і трансформуючого фактора росту β1 (TGF-β1) у дітей із ЮІА залежно від особливостей клінічного перебігу захворювання та отриманого лікування. Матеріали та методи. Обстежено 80 дітей із ЮІА, які знаходились на стаціонарному лікуванні в КП «Регіональний медичний центр родинного здоров’я» ДОР. Проведений ретроспективний аналіз медичної документації з оцінкою віку дитини в дебюті захворювання на ЮІА, тривалості його перебігу, клінічних особливостей і лікування. У подальшому під час виконання роботи проводили клінічне обстеження, оцінку стану здоров’я дітей, загальноклінічні, біохімічні, імуноферментні й імунологічні дослідження, ультразвукове дослідження суглобів та нирок. Для визначення структурних тубулярних маркерів KIM-1 і TGF-β1 у зразках сечі використовували імуноферментний аналіз. Результати. У середньому показник КІМ-1 дорівнював 0,9970 ± 0,1662 (0,98; 0,90–1,12) нг/мл, TGF-β1 — 20,26 ± 16,34 (14,02; 12,5–17,98) пг/мл. Середні значення KIM-1 варіювали залежно від форми ЮІА та ступеня активності захворювання. Водночас при високій активності ЮІА рівень KIM-1 був статистично значуще вищим (1,1510 ± 0,0806 нг/мл, p < 0,05 порівняно з ремісією). Подібна тенденція спостерігалася і при аналізі TGF-β1. Підвищений уміст KIM-1 асоціювався з високою активністю ЮІА, залученням ≥ 6 суглобів на момент обстеження, а також ураженням дрібних суглобів кистей рук та променево-зап’ясткових суглобів. Підвищений рівень TGF-β1 був статистично значуще асоційований із поліартритом, тривалістю ЮІА ≥ 6 років та активною стадією захворювання ≥ 4 років. Висновки. У нашому дослідженні виявлена статистично значуща залежність умісту біомаркерів KIM-1 та TGF-β1 від ступеня активності ЮІА. Статус антинуклеарних антитіл у пацієнтів з ЮІА не впливав на динаміку KIM-1 і TGF-β1. Підвищені рівні KIM-1 і TGF-β1 у сечі вказують на ризик структурного ураження нирок у пацієнтів з ЮІА. Факторами ризику є висока активність ЮІА, значне залучення суглобів, тривала активна стадія, наявність артеріальної гіпертензії, лікування НПЗП. Комбінація НПЗП та метотрексату підвищувала рівні KIM-1 і TGF-β1, що свідчило про нефротоксичну дію, тоді як комбінація метотрексату з імунобіологічними препаратами знижувала вміст біомаркерів.
Background. Juvenile idiopathic arthritis (JIA) is a heterogeneous group of diseases characterized by chronic joint inflammation in children under the age of 16 years. Kidney damage in JIA ranges from asymptomatic proteinuria to severe glomerulonephritis that can lead to chronic kidney disease. Given the above data, the assumption of an increased risk of early development of kidney damage in children with JIA is reasonable. The purpose was to analyze the risk factors for structural tubular lesions by studying the level of kidney injury molecule-1 (KIM-1) and transforming growth factor β1 (TGF-β1) in children with JIA, depending on the characteristics of the clinical course of the disease and the treatment received. Materials and methods. Eighty children with JIA who were undergoing inpatient treatment at the Regional Medical Center for Family Health of the State Regional Health Department were examined. A retrospective analysis of medical documentation was conducted to assess the child’s age at the onset of JIA, the duration of its course, clinical features, and treatment. Further, during the work, a clinical examination, assessment of the health of children, general clinical, biochemical, immunoenzymatic and immunological studies, ultrasound examination of joints and kidneys were performed. Structural tubular markers KIM-1 and TGF-β1 were measured in urine samples. Results. The average KIM-1 level was 0.9970 ± 0.1662 (0.98; 0.90–1.12) ng/ml, TGF-β1 — 20.26 ± 16.34 (14.02; 12.5–17.98) pg/ml. The average KIM-1 values varied depending on the form of JIA and the degree of disease activity. At the same time, with high JIA activity, the KIM-1 level was statistically significantly higher (1.1510 ± 0.0806 ng/ml, p < 0.05 compared to remission). A similar trend was observed when analyzing TGF-β1 levels. Elevated KIM-1 was associated with high JIA activity, involvement of ≥ 6 joints at the time of examination, and lesions of small joints of the hands and wrist joints. Elevated TGF-β1 was statistically significantly associated with polyarthritis, JIA duration of ≥ 6 years, and active disease stage of ≥ 4 years. Conclusions. Our study revealed a statistically significant relationship between the levels of KIM-1 and TGF-β1 biomarkers and the degree of JIA activity. The antinuclear antibodies status in patients with JIA did not affect the levels of KIM-1 and TGF-β1. Elevated content of KIM-1 and TGF-β1 in urine indicate the risk of structural kidney damage in patients with JIA. Risk factors are high JIA activity, significant joint involvement, prolonged active stage, the presence of hypertension, and NSAIDs treatment. The combination of NSAIDs with methotrexate increased the levels of KIM-1 and TGF-β1, which indicated a nephrotoxic effect, while the combination of methotrexate with immunobiological drugs decreased the levels of biomarkers.
ювенільний ідіопатичний артрит; нирки; діти; маркери раннього ураження нирок; КІМ-1; TGF-β1
juvenile idiopathic arthritis; kidneys; children; markers of early kidney damage; KIM-1; TGF-β1
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Thatayatikom A, Modica R, De Leucio A. Juvenile idiopathic arthritis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554605/.
- Heitman K, Alexander MS, Faul C. Skeletal muscle injury in chronic kidney disease — from histologic changes to molecular mechanisms and to novel therapies. Int J Mol Sci. 2024 May 8;25(10):5117. doi: 10.3390/ijms25105117.
- Kim SH. Renal involvement in pediatric rheumatologic disea–ses. Child Kidney Dis. 2022;26(1):18-24. doi: 10.3339/ckd.22.028.
- Giancane G, Alongi A, Ravelli A. Update on the pathogenesis and treatment of juvenile idiopathic arthritis. Curr Opin Rheumatol. 2017;29(5):523-529. doi: 10.1097/BOR.0000000000000417.
- Lucas GNC, Leitão ACC, Alencar RL, et al. Pathophysiological aspects of nephropathy caused by non-steroidal anti-inflammatory drugs. J Bras Nefrol. 2019;41(1):124-130. doi: 10.1590/2175-8239-JBN-2018-0107.
- Gicchino MF, Di Sessa A, Guarino S, et al. Prevalence of and factors associated to chronic kidney disease and hypertension in a cohort of children with juvenile idiopathic arthritis. Eur J Pediatr. 2021;180(2):655-661. doi: 10.1007/s00431-020-03792-4.
- Lousa I, Reis F, Beirão I, et al. New potential biomarkers for chronic kidney disease management — a review of the literature. Int J Mol Sci. 2020;22(1):43. doi: 10.3390/ijms22010043.
- Shao X, Tian L, Xu W, et al. Diagnostic value of urinary kidney injury molecule 1 for acute kidney injury: a meta-analysis. PLOS ONE. 2014;9(1):e84131. doi: 10.1371/journal.pone.0084131.
- Chimenz R, Chirico V, Basile P, et al. HMGB-1 and –TGFβ-1 highlight immuno-inflammatory and fibrotic processes before proteinuria onset in pediatric patients with Alport syndrome. J Nephrol. 2021;34(6):1915-1924. doi: 10.1007/s40620-021-01015-z.
- Moresco RN, Bochi GV, Stein CS, et al. Urinary kidney injury molecule-1 in renal disease. Clin Chim Acta. 2018 Dec;487:15-21. doi: 10.1016/j.cca.2018.09.011.
- Brilland B, Boud’hors C, Wacrenier S, et al. Kidney injury molecule 1 (KIM-1): a potential biomarker of acute kidney injury and tubulointerstitial injury in patients with ANCA-glomerulonephritis. Clin Kidney J. 2023 Apr 3;16(9):1521-1533. doi: 10.1093/ckj/sfad071.
- Yang L, Brooks CR, Xiao S, et al. KIM-1-mediated phagocytosis reduces acute injury to the kidney. J Clin Invest. 2015 Apr;125(4):1620-36. doi: 10.1172/JCI75417.
- Huang R, Fu P, Ma L. Kidney fibrosis: from mechanisms to therapeutic medicines. Signal Transduct Target Ther. 2023 Mar 17;8(1):129. doi: 10.1038/s41392-023-01379-7.
- Lawson J, Elliott J, Wheeler-Jones C, et al. Renal fibrosis in feline chronic kidney disease: known mediators and mechanisms of injury. Vet J. 2015 Jan;203(1):18-26. doi: 10.1016/j.tvjl.2014.10.009.
- Zhang Y, Dai Y, Raman A, et al. Overexpression of TGF-β1 induces renal fibrosis and accelerates the decline in kidney function in polycystic kidney disease. Am J Physiol Renal Physiol. 2020 Dec 1;319(6):F1135-F1148. doi: 10.1152/ajprenal.00366.2020.
- Tzavlaki K, Moustakas A. TGF-β signaling. Biomolecules. 2020 Mar 23;10(3):487. doi: 10.3390/biom10030487.
- Isaka Y. Targeting TGF-β signaling in kidney fibrosis. Int J Mol Sci. 2018 Aug 27;19(9):2532. doi: 10.3390/ijms19092532.
- Chen K, Zeng H, Togizbayev G, et al. New classification criteria for juvenile idiopathic arthritis. Int J Rheum Dis. 2023 Oct;26(10):1889-1892. doi: 10.1111/1756-185X.14813.
- Miyamae T, Tani Y, Kishi T, et al. Updated version of Japanese Childhood Health Assessment Questionnaire (CHAQ). Mod Rheumatol. 2020 Sep;30(5):905-909. doi: 10.1080/14397595.2019.1660027.
- Pierce CB, Muñoz A, Ng DK, et al. Age- and sex-dependent clinical equations to estimate glomerular filtration rates in children and young adults with chronic kidney disease. Kidney Int. 2021 Apr;99(4):948-956. doi: 10.1016/j.kint.2020.10.047.
- Instructions for use. HUMAN Kidney injury molecule-1 (KIM-1). Available from: https://www.mybiosource.com/kim-1-human-elisa-kits/kidney-injury-molecule-1/765516.
- Instructions for use. Transforming growth factor beta 1 (TGF-β1) ELISA. Available from: https://www.drg-diagnostics.de/files/eia-1864_ifu--tgf-beta1_2017-03-29_endeites.pdf.
- Swart JF, van Dijkhuizen EHP, Wulffraat NM, et al. Clinical juvenile arthritis disease activity score proves to be a useful tool in treat-to-target therapy in juvenile idiopathic arthritis. Ann Rheum Dis. 2018 Mar;77(3):336-342. doi: 10.1136/annrheumdis-2017-212104.
- Tang PC, Chan AS, Zhang CB, et al. TGF-β1 signaling: immune dynamics of chronic kidney diseases. Front Med (Lausanne). 2021;8:628519. doi: 10.3389/fmed.2021.628519.
- Song J, Yu J, Prayogo GW, et al. Understanding kidney injury molecule 1: a novel immune factor in kidney pathophysiology. Am J Transl Res. 2019;11(3):1219-1229.
- Yin C, Wang N. Kidney injury molecule-1 in kidney disease. Ren Fail. 2016 Nov;38(10):1567-1573. doi: 10.1080/0886022X. 2016.1193816.