
Журнал «Медицина неотложных состояний» Том 21, №2, 2025
Вернуться к номеру
Гендерні особливості перебігу токсоплазмозного енцефаліту у ВІЛ-інфікованих пацієнтів
Авторы: Велієва Т.А. (1), Бодня К.І. (1), Нартов П.В. (1, 2), Асоян І.М. (1), Макаренко В.Д. (1), Крохмаль І.В. (2)
(1) - Харківський національний медичний університет, м. Харків, Україна
(2) - Харківська обласна дитяча інфекційна клінічна лікарня, м. Харків, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
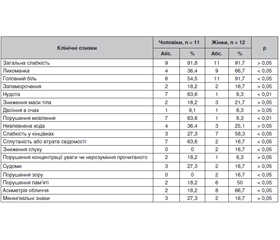
Актуальність. Токсоплазмозна інфекція в основному впливає на імунодефіцитних осіб, але є певні гендерні особливості, які можуть впливати на перебіг токсоплазмозного енцефаліту (ТЕ) у ВІЛ-інфікованих чоловіків та жінок. Метою роботи було проаналізувати гендерні особливості перебігу ТЕ у ВІЛ-інфікованих пацієнтів. Матеріали та методи. Здійснено ретроспективний аналіз гендерних особливостей перебігу ТЕ у 23 ВІЛ-інфікованих хворих. За гендерним складом чоловіків та жінок була майже однакова кількість: 11 (47,8 %) чоловіків та 12 (52,2 %) жінок. Вік хворих у середньому становив 37,50 ± 0,38 року. Середня кількість CD4+ лімфоцитів становила 102,5 ± 21,2 клітини/мкл, а навантаження РНК ВІЛ у плазмі при постановці діагнозу ТЕ становило 292 773,8 ± 113 180,0 копій/мл. Результати. Аналіз гендерних особливостей клінічного перебігу ТЕ у ВІЛ-інфікованих пацієнтів показав, що за низкою клінічних ознак мали місце суттєві відмінності між групами. Так, у чоловіків частіше виявлялись нудота (p < 0,01), порушення мовлення (p < 0,01) і сплутаність або втрата свідомості (p < 0,05), а серед жінок суттєво частіше діагностувалися лихоманка (p < 0,05), головний біль (p < 0,05), порушення пам’яті (p < 0,05), зниження слуху (p < 0,05), порушення зору (p < 0,05) і асиметрія обличчя (p < 0,05). При вивченні можливих чинників, які сприяють виникненню ТЕ у ВІЛ-інфікованих хворих (вмісту CD4+ та рівня IgG до T. gondii), встановлено, що організми чоловіків порівняно з жінками менш стійкі до токсоплазмозної інвазії, тому ТЕ розвивається у них на тлі навіть високого рівня CD4+ лімфоцитів і низької активності токсоплазмозної інвазії. Проте організми жінок більш стійкі, і ТЕ розвивається на тлі дуже низького вмісту CD4+ лімфоцитів і високої активності токсоплазмозної інвазії. Висновки. У чоловіків порівняно з жінками суттєво частіше діагностувалися клінічні прояви, що свідчать про локальні ураження мозку, а серед жінок суттєво частіше діагностувалися клінічні прояви, що свідчать про когнітивні та психічні розлади. ТЕ у жінок розвивається на тлі дуже низького вмісту CD4+ (≤ 10 клітин) і високого (≥ 401 МО/мл) рівня IgG до T. gondii, що спричиняє більш тяжкий клінічний перебіг хвороби порівняно з чоловіками.
Background. Toxoplasmosis mainly affects immunocompromised individuals, but there are certain gender characteristics that may influence the course of toxoplasmic encephalitis (TE) in HIV-infected men and women. The purpose was to analyze the gender characteristics of TE in HIV-infected patients. Materials and methods. A retrospective analysis of the gender characteristics of the TE course was performed in 23 HIV-infected patients. The gender composition was almost the same: 11 (47.8 %) men and 12 (52.2 %) women. The average age of patients was 37.50 ± 0.38 years. The average number of CD4+ lymphocytes was 102.5 ± 21.2 cells/μl, and the HIV RNA load in plasma at the diagnosis of TE was 292,773.8 ± 113,180 copies/ml. Results. Analysis of the gender characteristics of the clinical course of TE in HIV-infected patients showed that there were significant differences between the groups in a number of clinical signs. Thus, nausea (p < 0.01), speech impairment (p < 0.01) and confusion or loss of consciousness (p < 0.05) were more often detected in men, while fever (p < 0.05), headache (p < 0.05), memory impairment (p < 0.05), hearing loss (p < 0.05), visual impairment (p < 0.05) and facial asymmetry (p < 0.05) were significantly more often diagnosed among women. When studying possible factors that contribute to the occurrence of TE in HIV-infected patients (CD4+ content and IgG level to T. gondii), it was found that the body of men is less resistant to toxoplasmic invasion compared to women. Therefore, TE develops in them even against the background of high CD4+ lymphocytes and low activity of toxoplasmic invasion. The body of women is more resistant, and TE develops against the background of a very low content of CD4+ lymphocytes and high activity of toxoplasmic invasion. Conclusions. Thus, compared to women, clinical manifestations indicating local brain lesions were significantly more often diagnosed in men, while cognitive and mental disorders were significantly more common among women. TE in women develops on the background of a very low CD4+ count (≤ 10 cells) and a high (≥ 401 IU/ml) level of IgG to T. gondii, which causes a more severe clinical course of the disease compared to men.
токсоплазмозний енцефаліт; ВІЛ-інфекція; клінічні симптоми; гендерні особливості
toxoplasmic encephalitis; HIV infection; clinical symptoms; gender characteristics
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Elsheikha HM, Marra CM, Zhu X. Epidemiology, Pathophysiology, Diagnosis, and Management of Cerebral Toxoplasmosis. Clinical microbiology reviews. 2020;34(1):10-1128. doi: 10.1128/cmr.00115-19.
- Wesołowski R, Pawłowska M, Smoguła M, Szewczyk-Golec K. Advances and challenges in diagnostics of toxoplasmosis in HIV-infected patients. Pathogens. 2023;12(1):110. doi: 10.3390/pathogens12010110.
- Smith NC, Goulart C, Hayward JA, Kupz A, Miller CM, et al. Control of human toxoplasmosis. International journal for parasitology. 2021;51(2-3):95-121. doi: 10.1016/j.ijpara.2020.11.001.
- Schneider CA, Figueroa Velez DX, Orchanian SB, Shallberg LA, Agalliu D, et al. Toxoplasma gondii dissemination in the brain is facilitated by infiltrating peripheral immune cells. Mbio. 2022;13(6):e02838-22. doi: 10.1128/mbio.02838-22.
- Li Y, Zeng YM, Liu M, Lu YQ, Liu XY, et al. Development of a risk scoring system for prognostication in HIV-related toxoplasma encephalitis. BMC Infectious Diseases. 2020;20:1-8. doi: 10.1186/s12879-020-05651-x.
- Xiao J, Bhondoekhan F, Seaberg EC, Yang O, Stosor V, et al. Serological responses to Toxoplasma gondii and matrix antigen 1 predict the risk of subsequent Toxoplasmic Encephalitis in people living with human immunodeficiency virus (HIV). Clinical Infectious Di-seases. 2021;73(7):e2270-e2277. doi: 10.1093/cid/ciaa1917.
- Dian S, Ganiem AR, Ekawardhani S. Cerebral toxoplasmosis in HIV-infected patients: a review. Pathogens and global health. 2023;117(1):14-23. doi: 10.1080/20477724.2022.2083977.
- Cubas-Vega N, López Del-Tejo P, Baia-da-Silva DC, Sampaio VS, Jardim BA, et al. Early Antiretroviral Therapy in AIDS Patients Presenting With Toxoplasma gondii Encephalitis Is Associated With More Sequelae but Not Increased Mortality. Frontiersin Medicine. 2022;9:759091. doi: 10.3389/fmed.2022.759091.
- Prosty C, Hanula R, Levin Y, Bogoch II, McDonald EG, et al. Revisiting the evidence base for modern-day practice of the treatment of toxoplasmic encephalitis: a systematic review and meta-analysis. Clinical Infectious Diseases. 2023;76(3):e1302-1319. doi: 10.1093/cid/ciac645.
- Dubey JP, Cerqueira-Cézar CK, Murata FHA, Kwok OCH, Yang YR, et al. All about toxoplasmosis in cats: the last decade. Veterinary. Parasitology. 2020;283:109145. doi: 10.1016/j.vetpar.2020.109145.
- Bollani L, Auriti C, Achille C, Garofoli F, De Rose DU, et al. Congenital toxoplasmosis: the state of the art. Frontiers in pediatrics. 2022;10:894573. doi: 10.3389/fped.2022.894573.
- Durieux MF, Lopez JG, Banjari M, Passebosc-Faure K, Brenier-Pinchart MP, et al. Toxoplasmosis in patients with an autoimmune disease and immunosuppressive agents: A multicenter study and literature review. PLоS Neglected Tropical Diseases. 2022;16(8):e0010691. doi: 10.1371/journal.pntd.0010691.
- Mouveaux T, Roger E, Gueye A, Eysert F, Huot L, et al. Primary brain cell infection by Toxoplasma gondii reveals the extent and dynamics of parasite differentiation and its impact on neuron biology. Open biology. 2021;11(10):210053. doi: 10.1098/rsob.210053.
- Safarpour H, Cevik M, Zarean M, Barac A, Hatam-Nahavandi K, et al. Global status of Toxoplasma gondii infection and associated risk factors in people living with HIV. Aids. 2020;34(3):469-474. doi: 10.1097/QAD.0000000000002424.
- Fard SA, Khajeh A, Khosravi A, Mirshekar A, Masoumi S, et al. Fulminant and diffuse cerebral toxoplasmosis as the first manifestation of HIV infection: a case presentation and review of the literature. The American journal of case reports. 2020;21:e919624-1. doi: 10.12659/AJCR.919624.
- Lyons MR, Arantes T, Vieira BR, Furtado JM, Smith JR. Impact of gender on clinical features and outcomes of ocular toxoplasmosis. British Journal of Ophthalmology. 2024;108:710-714. doi: 10.1136/bjo-2023-323227.
- Dwinata IM, Widyadharma IPE, Dewi PR, Tedyanto EH. Risk factors of cerebral toxoplasmosis in HIV patients: a systematic review. Romanian Journal of Neurology. 2021;20(3):305-310. doi: 10.37897/RJN.2021.3.7.