
Международный неврологический журнал №5 (107), 2019
Вернуться к номеру
Зміни рухових функцій у дітей iз церебральним паралічем після курсу інтенсивної нейрофізіологічної реабілітації: сліпе дослідження
Авторы: O. Kachmar (1), I. Mysula (2), A. Kushnir (1), T. Voloshyn (1), O. Matiushenko (1), M. Hasiuk (1), M. Hordiyevych (1)
1 - International Rehabilitation Clinic, Truskavets, Ukraine
2 - State Institution of Higher Education “I. Horbachevsky Ternopil National Medical University”, Ternopil, Ukraine
Рубрики: Неврология
Разделы: Клинические исследования
Версия для печати
Актуальність. Розробка сучасних інтенсивних технологій реабілітації пацієнтів iз дитячим церебральним паралічем (ДЦП), спрямованих на покращення різних аспектів функціонування дитини, є актуальним завданням фахівців-практиків та дослідників. Одним iз таких підходів є система інтенсивної нейрофізіологічної реабілітації (СІНР), що поєднує різнопланові методи лікування, спрямовані на досягнення функціональних цілей та об’єднані в один інтенсивний курс. Метою дослідження була оцінка змін великих моторних функцій, спастичності м’язів та об’єму пасивних рухів у суглобах у пацієнтів із спастичними формами ДЦП після двотижневого курсу лікування за СІНР. Матеріали та методи. Одностороннє сліпе дослідження було проведене в групі з 57 дітей віком від 4 до 12 років зі спастичними формами ДЦП, які проходили курс лікування у спеціалізованій реабілітаційній клініці. Пацієнтів обстежували до та після двотижневого курсу лікування за СІНР, що включав численні втручання загальною тривалістю 4–5 годин на добу. Виконання пацієнтом завдань тесту щодо оцінки великих моторних функцій (GMFM-66) записувалося на відео та оцінювалося незалежно двома фахівцями. Час запису (до чи після лікування) був замаскований. Об’єм пасивних рухів в суглобах нижніх кінцівок оцінювали за допомогою гоніометра, м’язову спастичність — модифікованої шкали Ашворта. Результати. Після курсу лікування за СІНР відмічене статистично вірогідне підвищення результату тесту GMFM-66 з 58,8 до 60,2 бала, iз середньою різницею 1,4 ± 2,9 бала. Істотне покращення об’єму пасивних рухів було відзначене при виконаннi 5 з 7 рухiв, найбільш виражене при приведенні кульшового суглоба — в середньому на 8,0 ± 5,8 градуса та тильному згинанні стопи — на 8,0 ± 6,1 градуса. Зниження м’язового тонусу спостерігалось у всіх інших м’язових групах, що оцінювалися. Статистично вірогідне зниження спастичності відзначене в згиначах стегна, iз середнім зниженням на 0,25 пункту за шкалою Ашворта (95% довірчий інтервал (ДІ) = 0,06–0,44), та аддукторах стегна — на 0,30 пункту (95% ДІ = 0,08–0,51). Висновки. Після двотижневого курсу лікування за СІНР зареєстровані покращення великих моторних функцій, збільшення об’єму пасивних рухів і зниження спастичності м’язів нижніх кінцівок. Інтенсивна реабілітація за СІНР потребує проведення подальших досліджень, у тому числі рандомізованих контрольованих.
Актуальность. Разработка современных интенсивных технологий реабилитации пациентов с детским церебральным параличом (ДЦП), направленных на улучшение различных аспектов функционирования ребенка, является актуальной задачей специалистов-практиков и исследователей. Одним из таких подходов является cистема интенсивной нейрофизиологической реабилитации (СИНР), которая сочетает разноплановые методы лечения, направленные на достижение функциональных целей и объединенные в один интенсивный курс. Целью исследования была оценка изменений больших моторных функций, мышечной спастичности и объема пассивных движений в суставах у пациентов со спастическими формами ДЦП после двухнедельного курса лечения по СИНР. Материалы и методы. Одностороннее слепое исследование было проведено в группе из 57 детей возрастом от 4 до 12 лет со спастическими формами ДЦП, которые проходили курс лечения в специализированной реабилитационной клинике. Пациентов обследовали до и после двухнедельного курса лечения по СИНР, который включал многочисленные вмешательства общей продолжительностью 4–5 часов в сутки. Выполнение пациентом заданий теста по оценке больших моторных функций (GMFM-66) записывалось на видео и оценивалось независимо двумя специалистами. Время записи (до или после лечения) было замаскировано. Объем пассивных движений в суставах нижних конечностей оценивали с помощью гониометра, мышечную спастичность — модифицированной шкалы Ашворта. Результаты. После курса лечения по СИНР отмечено статистически достоверное повышение результата теста GMFM-66 с 58,8 до 60,2 балла, со средней разницей в 1,4 ± 2,9 балла. Существенное увеличение объема пассивных движений отмечено при выполнении 5 из 7 движений, наиболее выраженное при приведении тазобедренного сустава — в среднем на 8,0 ± 5,8 градуса и тыльном сгибании стопы — на 8,0 ± 6,1 градуса. Снижение мышечного тонуса наблюдалось во всех оцениваемых мышечных группах. Статистически значимое снижение спастичности отмечено в сгибателях бедра, со средним уменьшением на 0,25 пункта по шкале Ашворта (95% доверительный интервал (ДИ) = 0,06–0,44), и аддукторах бедра — на 0,30 пункта (95% ДИ = 0,08–0,51). Выводы. После двухнедельного курса лечения по СИНР зарегистрировано улучшение больших моторных функций, увеличение объема пассивных движений и снижение спастичности мышц нижних конечностей. Интенсивная реабилитация по СИНР требует проведения дальнейших исследований, в том числе рандомизированных контролируемых.
Background. Modern intensive interventions addressing multiple challenges in children with cerebral palsy are attracting clinicians’ and researchers’ attention. One of such methods is the intensive neurophysiological rehabilitation system (INRS) — a combination of interventions focusing on different functional goals, merged into one intensive course. The purpose of the study was to assess changes in gross motor functions, muscle spasticity and passive range of motion (PROM) in children with spastic forms of cerebral palsy (CP) after the two-week of treatment course with INRS. Materials and methods. A single-arm, single-blind pre-post study was conducted among 57 children aged 4 to 12 years with spastic CP, admitted for treatment to the tertiary care center. Patients were examined before and after the two-week course using INRS, which included multiple interventions totalling 4–5 hours of treatment daily. The Gross Motor Function Measure-66 (GMFM-66) tasks were video-recorded and evaluated independently by two investigators. The time of recordings (baseline or post-intervention) was masked. PROM in the lower extremity joints was assessed with a manual goniometer, muscle spasticity — with the Modified Ashworth scale. Results. GMFM-66 scores after INRS use increased statistically significantly from 58.8 to 60.2 points, with a mean difference of 1.4 ± 2.9 points. Substantial improvement in PROM was noted for 5 of 7 movements; the most substantial improvement was observed in hip abduction — an average of 8.0 ± 5.8° and foot dorsiflexion — 8.0 ± 6.1°. Reduction of the muscle tone was observed in all measured muscle groups. Statistically significant decrease of spasticity was noted in hip flexors, with an average reduction of 0.25 scale steps (95% confidence interval (CI) = 0.06–0.44), and hip adductors — 0.30 steps (95% CI = 0.08–0.51). Conclusions. Improvements of gross motor functions, an increase of PROM in the lower extremities and reduction of muscle spasticity have been detected after the two-week course with INRS. Intensive treatment using INRS requires further studies, including randomized controlled ones.
церебральний параліч; реабілітація; фізична терапія; рухові порушення; м’язова спастичність
церебральный паралич; реабилитация; физическая терапия; двигательные нарушения; мышечная спастичность
cerebral palsy; rehabilitation; physical therapy; motor disorders; muscle spasticity
Introduction
Cerebral palsy (CP) is a group of permanent disorders of movement and posture, causing activity limitation that is attributed to nonprogressive disturbances of brain deve–lopment. Motor disorders are often accompanied by disturbances of sensation, perception, cognition, communication, and behavior, as well as seizure disorders [1].
According to the recently introduced International Classification of Functioning (ICF) Core Sets for children with CP, particular attention is directed towards multiple limitations in the Body Functions domain (joint mobility, muscle tone, voluntary movement, pain, intellectual functions) and Activities and Participation domains (body position, fine hand use, walking, moving around, interpersonal interactions and family relationships) [2]. To improve the functioning and quality of life of children with CP, it is important to implement a comprehensive treatment program addressing multiple challenges in different ICF domains [3].
As a consequence of the rapid growth in CP research in the last decade, safer and more effective interventions for children with cerebral palsy have been introduced. At least 64 different interventions for cerebral palsy aimed at different dysfunctions have been presented and analyzed in the systematic review [4].
Particular attention is directed towards intensive treatments; they are developing rapidly and are supported by a growing amount of evidence, indicating that therapies of higher intensity are more effective. A Cochrane review on constraint–induced movement therapy indicates that this intensive intervention is more effective for improving unimanual hand functions than a low–intensity alternative [5]. A quasi–randomized trial of the intensive upper and lower extremity training providing 6.5 intensive intervention hours per day over 13 consecutive days reports significant improvement in gross and fine motor functions in children with bilateral CP [6]. A large cohort study of 442 Norwegian children based on the CP register indicates that a more frequent physical therapy is associated with increased gross motor improvement [7].
So, the attention of both researchers and clinicians is focused on the exploration of high–intensity and function–oriented treatments addressing multiple limitations in children with CP. One of such approaches is an intensive neurophysio–logical rehabilitation system (INRS) — a combination of different interventions addressing different functional goals in one intensive course [8]. This treatment system is also known by the name of its author as the Kozyavkin method.
The treatment program is tailored individually accor–ding to the patient’s condition and comprises the following components: physical therapy, occupational therapy, full body massage, spinal manipulative therapy, reflexotherapy, strength training, computer game therapy, suit therapy, vibration therapy, treadmill training and group session of rhythmic gymnastics. Intensive intervention includes 4–5 hours of daily treatment over two weeks.
Recent retrospective analysis of medical records of children undergoing treatment with INRS indicates the improvement of gross motor function, decrease of muscle spasticity, development of fine motor skills and other positive changes achieved in a relatively short period of time [9].
The purpose of the study. The present exploratory study was conducted to assess changes in gross motor function in children with spastic forms of cerebral palsy after the two–week treatment with INRS in a single–blind study. A secon–dary purpose of the study was to assess the changes in muscle spasticity and passive range of motion (PROM) in the lower extremity joints.
Materials and methods
Study design
A single–arm, single–blind pre–post study design was used. Patients admitted for treatment to the tertiary care rehabilitation center after screening examination were invited for participation. Gross motor function, passive range of motion, and spasticity assessments were performed before and after a two–week treatment course, with patients serving as their own controls.
Performance of gross motor functions before and after the treatment was recorded on video and reviewed independently by two blinded reviewers, not knowing which (pre or post) video they were rating. Assessment of the muscle spasticity and range of motion in joints was performed by the physician involved in the treatment of the patient, so this part of the study was not blinded.
Participants
All participants were patients of the International Clinic of Rehabilitation. To be eligible for the study, children had to be local residents, 4 to 12 years of age, with spastic bilate–ral cerebral palsy and Gross Motor Function Classification System (GMFCS) levels II–IV.
Exclusion criteria were: severe epileptic syndrome, severe mental retardation and inability to understand and comply with instructions, ongoing antispastic medication intake, botox injections during the preceding year, and uncooperative behavior.
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the commission of ethics of the International Clinic of Rehabilitation (protocol number N–2014–01–20). Participants and their legal representatives received comprehensive information about the procedures and study design; written informed consent was obtained from legal representatives. Where appropriate, based on age and cognitive abilities, participants were asked to give verbal assent.
Sixty–one patients have been included in the study and underwent baseline assessment. Later, 4 children have been excluded from the study due to the somatic illness develo–ping during the treatment or non–compliance with the study requirements. Hence, the data of 57 children were used.
During the study, no complications or side effects have been observed by medical specialists or reported by the patients/parents.
Demographic characteristics of the patients are presented in Table 1. The average age of the children was 7.1 years (standard deviation (SD) 2.2), among them, 58 % were males, 46 % patients had GMFCS level III and 49 % — Manual Ability Classification System (MACS) level II.
/16-1.jpg)
Outcome measures
The primary outcome measure was the change in the gross motor function score measured using the Gross Motor Function Measure–66 (GMFM–66) [10, 11]. The GMFM–66 is a valid and reliable tool consisting of 66 activities that range in difficulty from lying and reaching for a toy to walking, running, and jumping. Depending on the available time and patient’s motor ability, some activities may be skipped, but at least 13 test items must be performed for accurate results. Performance on each item is scored on a four–point scale. A score 3 indicates that a child completes 100 % of the activity, 0 — that he/she is unable to commence any part of it. Specific sco–ring descriptors for each item are detailed in the user’s manual. Individual item scores are converted into the total score with the dedicated software Gross Motor Ability Estimator.
Each GMFM–66 test session was video–recorded, and the recordings were scored independently by two trained investigators. When there were discrepancies, the item was reviewed and scored to reach a consensus. The investigators were blinded to whether they watched a pre– or post–treatment video recording in order to reduce bias.
Secondary outcome measures included the change in PROM and muscle spasticity. PROM was measured with a hand–held goniometer in a standardized way [12]. Following movements have been assessed: 1) hip abduction; 2) hip flexion; 3) hip extension; 4) knee flexion (popliteal angle); 5) knee extension; 6) dorsiflexion of the foot with flexed knee; 7) dorsiflexion of the foot with the extended knee. For each child, we measured both the left and right side.
The Modified Ashworth Scale (MAS) was used to measure muscle spasticity. The assessor evaluated the resistance to rapid passive stretch of the tested muscle and assigned a score on a six–point scale (0, 1, 1+, 2, 3, 4), where 0 indicates normal muscle tone and 4 stands for rigidity [13]. In the calculations we replaced the point names (0, 1, 1+, 2, 3, 4) with ordinal numbers (0, 1, 2, 3, 4, 5). We measured spasticity in the hip flexors, hip adductors, knee flexors, knee extensors, and foot dorsiflexors on both sides.
Statistical analysis
Data analysis was performed using IBM SPSS v23 software. Normality of distribution was evaluated using the Kolmogorov–Smirnov test. GMFM–66 score and PROM values were compared using the paired sample t–test. Relationship between age and GMFM–66 score was calculated using Pearson correlation coefficient. Wilcoxon signed–rank test for related samples was used for calculation of MAS changes.
Intervention
All patients underwent a two–week rehabilitation course according to the intensive neurophysiological rehabilitation system. The course includes 4 to 5 hours of daily training. Treatment plan is worked out individually depending on the patient’s condition and incorporates some of the following components:
— physical therapy aimed at gross motor training is performed daily for 30 minutes and includes individua–lized exercises to improve gross motor function, increase mobility, and strengthen the muscles;
— occupational therapy is focused on the development of skills necessary for the performance of everyday activities including play and self–care activities such as dressing, grooming and feeding, and fine motor tasks such as writing and drawing. The treatment program includes both uni– and bimanual tasks;
— full body massage lasts for 60 min a day and incorporates classic, deep tissue, periosteal massage, trigger point therapy and muscle stretching techniques;
— spinal manipulative therapy (2–5 min/day) is a variation of the spinal manipulation carried out in lumbar, thoracic and cervical regions using high–velocity, low–amplitude thrust techniques;
— joint mobilization techniques (20 min/day) are aimed at improving range of motion, decreasing pain and improving function of the extremities;
— paraffin and wax applications (20 min/day) include thermal effects on muscles and joints by enveloping different muscle groups and joints in warm paraffin and wax wraps;
— reflexotherapy (10 min/day) includes low–current electric stimulation of the trigger and acupuncture points using a special portable device;
— strength training (mechanotherapy) (15 min/day) is aimed to build up muscle strength and endurance using machines adjusted for resistance;
— computer game therapy (15 min/day) using different game consoles like Nintendo Wii Fit with ba–lance board, Xbox with the Kinect motion sensor, and games developed specifically for children with motor problems [8];
— suit therapy (30 min/day) is performed using a special Spiral suit that creates external forces for correction of the movements and posture of the patient and helps to attain new movement patterns [14];
— vibration therapy (10 min/day) utilizes high–frequency, low–magnitude vibration to promote bone and muscle strength;
— treadmill training (15 min/day) with support of a physiotherapist who corrects the gait manually;
— group session of rhythmic gymnastics based on the game with the use of music and dancing.
A detailed description of the treatment system inclu–ding indications and contraindications is presented in the rehabilitation manual [8].
Results
Gross motor functions
Mean values of the GMFM–66 score with standard deviation at baseline and post–intervention assessment are summarized in Table 2.
/18-1.jpg)
Table 2 includes data for the whole group and is also divided by GMFCS level or by age group. An increase of the mean GMFM–66 score by 1.4 ± 2.9 points from 58.8 to 60.2 after the treatment course with INRS was noted for the whole group. Paired sample t–test showed that this change was statistically significant (p < 0.05).
The most substantial improvement was noted in children with GMFCS level IV, where the score increased by 2.3 ± 2.8 points, from 46.1 to 48.4 (p < 0.05).
Splitting the group by age was less informative, since the standard deviation of the GMFM–66 score for age subgroups was considerably higher. The significant change was noted only in the 7–9–year age group.
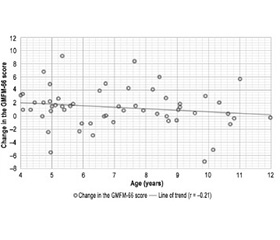
We have calculated dependence between motor improvement and age. Fig. 1 presents a scatterplot of the change in GMFM–66 score depending on the age. Each point represents a score change in one child. Line of trend reflects very small negative correlation, Spearman’s correlation coefficient equals –0.21, indicating that younger children experience a slightly greater motor improvement.
/18-2.jpg)
Passive range of motion
The data of PROM in joints are presented in Table 3. Mean values with standard deviation were calculated for baseline and post–intervention measurements for all the joints. Since all the patients had bilateral CP and both extremities were evaluated, the sample size for PROM measurements and spasticity tests included 114 observations.
/18-3.jpg)
An increase in PROM, ranging from 2 to 8°, was observed in all joints. The greatest changes were observed in hip abduction and foot dorsiflexion with extended knee, where PROM increased by 8.0 ± 5.8 and 8.0 ± 6.1°, respectively. Also, statistically significant changes were noted in the popliteal angle and foot dorsiflexion with flexed knees. The smallest improvement was observed in knee extension.
Spasticity
The data on muscle spasticity before and after the two–week treatment course are presented in Table 4. Scores of muscle spasticity (MAS) are ordinal variables, so we presented the median and interquartile range values. We also included mean values of the MAS score to clearly illustrate the data trends.
/19-1.jpg)
The pre/post difference was calculated using Wilcoxon signed–rank test for dependent samples, and results are presented as a 95% confidence interval and significance (p–value.) A p–value below 0.05 was considered statistically significant and is marked with an asterisk.
Statistically significant decrease of spasticity was noted in hip flexors, with an average reduction by 0.25 scale steps (95% CI = 0.06–0.44), and hip adductors — by 0.30 steps (95% CI = 0.08–0.51). Decrease of knee flexor spasticity was not statistically significant (p = 0.067).
Muscle tone improvement was also noted in other measured muscle groups but did not reach 95% significance.
Discussion
The primary aim of our study was to evaluate changes in gross motor functions occurring in children with CP after the two–week course of intensive and multicomponent rehabilitation treatment with INRS.
Advantages of intensive rehabilitation were reported by different research groups [6, 7, 15, 16]. In the pre–sent study, participants received high–intensity treatment (5 days, 20 hours per week) with a total number of treatment modalities used ranging between 10 and 13.
The first part of the study was an assessment of gross motor functions with GMFM–66. To reduce possible bias when interpreting the results, a single–blind scoring was used. Video recordings of the patients performing GMFM–66 tasks were scored independently by two trained researchers. The dates of video recordings were removed from the file in advance, so the researchers were unaware of where the recordings had been performed before or after the treatment course.
Study results demonstrated a statistically significant increase in the GMFM–66 score by a mean of 1.4 points (p < 0.05). While answering how clinically those finding are, we should refer to the multicenter study conducted in the Shriners hospital for children [17]. By using a systematic method for establishing the minimum clinically important difference on a sample of 381 children, they concluded that a change of 0.8 points in the GMFM–66 test should be interpreted as a medium–size effect and 1.3 points — as a large effect. So, the mean difference of 1.4 points on GMFM–66 in the whole group can be interpreted as a large change. The putative mechanisms, which could have caused the medium–size to large effect on gross motor functions, could include neuroplasticity impact, motor learning, and increased strength as a result of intensive functional treatment [6, 16].
We observed slightly greater improvements in gross motor skills in younger children compared to older ones. A small negative correlation between the change of the GMFM–66 score and age of the child was noted (Spearman’s correlation coefficient = –0.21). Similar results have been described by other researcher, indicating a better response to treatment in younger children with cerebral palsy [18]. These data support the idea of applying early rehabilitation programs for children with CP or at high risk of CP development [19].
The second part of the study was aimed at evaluation of the changes in muscle spasticity and passive range of motion in lower extremity joints. Statistically significant pre/post difference of PROM was observed in the hip and ankle joints (Table 3). The difference in PROM measurements is associated with statistically significant changes in spasticity, detected in the lower extremity muscle groups (Table 4). As spasticity is a factor that directly affects acquisition of new motor skills, even subtle reduction of spasticity is beneficial for patients with cerebral palsy [20].
In this pre/post study, we decided to assess the effect of the intensive multimodal treatment on the Body structure (muscle spasticity, PROM) and Activity (GMFM–66 score) domains of the ICF [3]. We found that more frequent rehabilitation with different components is associated with improvement in the aforementioned domains. In future investigations, we will also include the participation domain for a more comprehensive understanding of how INRS affects the key aspects of the quality of life in children with CP.
Limitations of the study
An important limitation of our study was its pre/post design without control group. We decided not to include control group due to possible ethical concerns. In the near future, we plan to perform a double–blind randomized control trial to achieve more conclusive evidence.
Another limitation was due to the peculiarities of the MAS and goniometry. Several studies have reported goniometry measurement error of 10–15° and greater if different testers perform the measurement [21, 22]. We attempted to handle this issue by every assessment being performed by the same evaluator. However, even with such preconditions, there is still the risk of possible error [23].
Conclusions
Improvements of gross motor functions, increase in PROM and reduction of muscle spasticity in lower extremities were noted in children with CP after the two–week intensive multimodal treatment course with INRS.
More detailed investigation of the treatment with INRS requires further studies, including double–blind randomized controlled trials.
Conflicts of interests. Authors declare the absence of any conflicts of interests that might be construed to influence the results or interpretation of their manuscript.
1. Rosenbaum P., Paneth N., Leviton A., Goldstein M., Bax M., Damiano D., Dan B., Jacobsson B. A report: the definition and classification of cerebral palsy. Dev. Med. Child Neurol. 2007, Suppl. Feb. 109. 8–14.
2. Schiariti V., Selb M., Cieza A., O’Donnell M. International Classification of Functioning, Disability and Health Core Sets for children and youth with cerebral palsy: a consensus meeting. Dev. Med. Child Neurol. 2015. 57(2). 149–158.
3. World Health Organization. International classification of functioning, disability and health: ICF. Geneva: World Health Organization, 2001.
4. Novak I., McIntyre S., Morgan C., Campbell L., Dark L., Morton N., Goldsmith S. A systematic review of interventions for children with cerebral palsy: state of the evidence. Dev. Med. Child Neurol. 2013. 55(10). 885–910.
5. Hoare B.J., Wallen M.A., Thorley M.N., Jackman M.L., Ca–rey L.M., Imms C. Constraint-induced movement therapy in children with unilateral cerebral palsy. Cochrane Database of Systematic Reviews. 2019. 4.
6. Bleyenheuft Y., Ebner–Karestinos D., Surana B., Paradis J., Sidiropoulos A., Renders A., Gordon A.M. Intensive upper- and lower-extremity training for children with bilateral cerebral palsy: a quasi-randomized trial. Dev. Med. Child Neurol. 2017. 59(6). 625–633.
7. Størvold G.V., Jahnsen R.B., Evensen K.A.I., Bratberg G.H. Is more frequent physical therapy associated with increased gross motor improvement in children with cerebral palsy? A national prospective cohort study. Disability and Rehabilitation. 2018. 1–9.
8. Kozyavkin V.I., Babadagly M.O., Lun G.P., Kachmar O.O., Hordievych S.M., Lysovych V.I., Voloshyn B.D. Intensive Neurophy–siological Rehabilitation System — the Kozyavkin method. A manual for rehabilitation specialists. Lviv: Design studio Papuga, 2012.
9. Kozyavkin V.I., Kachmar O.O., Lysovych V.I. A retrospective analysis of the results of treatment with Intensive Neurophysiological Rehabilitation System. International Neurological Journal. 2018. 3(97). 13–22.
10. Russell D.J., Rosenbaum P.L., Wright M., Avery L.M. Gross motor function measure (GMFM–66 & GMFM–88) user’s manual. Vol. 159. London: Mac Keith Press, 2002.
11. Kachmar O.O., Kozyavkin V.I., Hordiievych M.S. Reliability of the Ukrainian version of the Gross motor function classification system. International Neurological Journal. 2010. 5. 357.
12. Norkin C.C., White D.J. Measurement of joint motion: a guide to goniometry. 5th ed. Philadelphia: Davis Company, 2016.
13. Bohannon R.W., Smith M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Physical Therapy. 1987. 67(2). 206–207.
14. Kozijavkin V., Kachmar O. Correction of movement utilizing the “Spiral” suit — an important part of the Kozijavkin method. Cerebral Palsy Magazine. 2004. 14–18.
15. Evans–Rogers D.L., Sweeney J.K., Holden–Huchton P., Mullens P.A. Short–term, intensive neurodevelopmental treatment program experiences of parents and their children with disabilities. Pediatric Physical Therapy. 2015. 27(1). 61–71.
16. Roelofsma R., Rameckers E. The effect of a functional intensive intervention program on self–care in children with cerebral palsy: a case study. Int. J. Brain Disord. Treat. 2017. 3.
17. Oeffinger D. et al. Outcome tools used for ambulatory children with cerebral palsy: responsiveness and minimum clinically important differences. Dev. Med. Child Neurol. 2008. 50(12). 918–925. https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1469–8749.2008.03150.x.
18. Ko J. Sensitivity to functional improvements of GMFM–88, GMFM–66, and PEDI mobility scores in young children with cerebral palsy. Percept. Mot. Skills. 2014 Aug. 119(1). 305–19.
19. Novak I. Evidence–based diagnosis, health care, and rehabilitation for children with cerebral palsy. J. Child Neurol. 2014 Aug. 29(8). 1141–56.
20. Katusic A., Alimovic S. The relationship between spasticity and gross motor capability in nonambulatory children with spastic cerebral palsy. Int. J. Rehabil. Res. 2013 Sep. 36(3). 205–10.
21. Stuberg W.A., Fuchs R.H., Miedaner J.A. Reliability of goniometric measurements of children with cerebral palsy. Dev. Med. Child Neurol. 1988. 30. 657–66.
22. MсDowell B.C., Hewitt V., Nurse A., Weston T., Baker R. The variability of goniometric measurements in ambulatory children with spastic cerebral palsy. Gait & Posture. 2000. 12. 114–21.
23. Nordmark E., Hägglund G., Lauge–Pedersen H., Wagner P., Westbom L. Development of lower limb range of motion from early childhood to adolescence in cerebral palsy: a population–based study. BMC Medicine. 2009. 7(1).