
Архив офтальмологии Украины Том 11, №2, 2023
Вернуться к номеру
Фактори ризику і прогноз оперативного лікування регматогенного відшарування сітківки
Авторы: Жабоєдов Д.Г. (1), Жук А.М. (2)
(1) — Національний медичний університет імені О.О. Богомольця, м. Київ, Україна
(2) — ТОВ «Британський офтальмологічний центр», м. Київ, Україна
Рубрики: Офтальмология
Разделы: Клинические исследования
Версия для печати
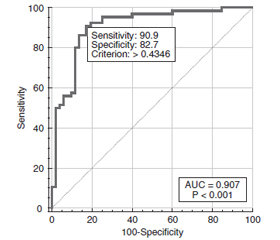
Актуальність. Основною метою лікування регматогенного відшарування сітківки (РВС) є відновлення анатомо-топографічних співвідношень у задньому полюсі ока, відмежування розривів за рахунок формування хоріоретинальних спайок і видалення проліферативних мембран, а також відновлення зорових функцій. Ефективність хірургії широко варіює незалежно від обраного методу лікування і знаходиться в межах від 37 до 95 %. Матеріали та методи. Під спостереженням перебували 124 пацієнти (124 ока) з РВС у поєднанні з віковою катарактою. 1-шу групу спостереження становили 60 пацієнтів (60 очей), яким виконували закриту субтотальну вітректомію з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки і факоемульсифікацією катаракти з імплантацією інтраокулярної лінзи (при подальшому аналізі позначено як метод операції 1). 2-гу групу спостереження становили 64 пацієнти (64 ока), яким виконували таке саме оперативне втручання, але тампонаду вітреальної порожнини проводили із застосуванням силіконового масла (при подальшому аналізі позначено як метод операції 2). Для виявлення факторів, пов’язаних з результатом лікування, використано метод побудови моделей логістичної регресії з використанням пакетів MedStat і MedCalc v.15.1 (MedCalc Software bvba). Аналіз проводився для факторів ризику, які були визначені на момент проведення операції. Відбір предикторів регресійної моделі здійснювали методом максимальної правдоподібності з покроковим виключенням змінних. Отримані регресійні моделі оцінювали при побудові діаграм операційних характеристик (ROC-аналіз). Як критерій адекватності моделі розраховували площу під кривою операційних характеристик з інтервальною оцінкою (AUC). Результати. Факторами ризику відсутності поліпшення стану в результаті оперативного лікування РВС через 1 рік після втручання були вік, давність відшарування сітківки, стадія С проліферативної вітреоретинопатії (ПВР), метод операції і показник суми локальних дефектів полів зору (PSD). Факторами ризику погіршення стану були вік, стать, давність ВС, вид розриву сітківки, стадія С ПВР, метод операції і PSD. У нашому дослідженні встановлений більший ризик невдалого лікування РВС для чоловіків, ніж для жінок. Прогностична модель невдалого хірургічного лікування РВС була побудована на трьох факторах ризику: видалення кришталика (p = 0,046), ПВР стадії C (p = 0,039) і ступінь відшарування (p < 0,001) і мала велику прогностичну цінність (площа під ROC-кривою становила 0,8399). Визначення прогнозу погіршення і відсутності поліпшення стану через 1 рік після оперативного лікування також мало досить високі показники якості моделі (AUC = 0,817 і 0,907 відповідно).
Background. The main purpose of treatment for rhegmatogenous retinal detachment (RRD) is to restore anatomical and topographical relations in the posterior pole of the eye, to demarcate tears due to the formation of chorioretinal adhesions and to remove proliferative membranes, as well as to restore visual functions. The effectiveness of surgery varies widely, regardless of the chosen treatment method, and ranges from 37 to 95 %. Materials and methods. One hundred and twenty-four patients (124 eyes) with RRD combined with age-related cataract were under observation. The first group consisted of 60 patients (60 eyes) who underwent closed subtotal vitrectomy with vitreous tamponade using a C3F8 gas-air mixture, endolaser coagulation of the retina, and phacoemulsification with an intraocular lens implantation (in further analysis, it was designated as surgical method 1). The second observation group included 64 patients (64 eyes), who underwent the same intervention, but vitreous tamponade was performed with the use of silicone oil (surgical method 2). To identify factors related to the treatment outcome, the method of building logistic regression models using MedStat and MedCalc v.15.1 packages (MedCalc Software bvba) was used. The analysis was carried out for risk factors that were determined at the time of the operation. The selection of predictors of the regression model was carried out by the method of maximum likelihood with stepwise exclusion of variables. The resulting regression models were evaluated by constructing diagrams of operating characteristics (receiver operator characteristic (ROC) analysis). As a criterion of model adequacy, the area under the ROC curve (AUC) with interval estimation was calculated. Results. The risk factors for not improving the state as a result of surgical treatment for RRD one year after the intervention were age, age of retinal detachment, stage C of proliferative vitreoretinopathy (PVR), method of surgery and pattern standard deviation. The risk factors for deterioration were age, gender, age of retinal detachment, type of retinal tear, stage C of PVR, method of surgery and pattern standard deviation. In our study, a risk of unsuccessful treatment for RRD was higher in men than in women. The prognostic model of unsuccessful surgical treatment for RRD was built on three risk factors: lensectomy (p = 0.046), stage C of PVR (p = 0.039), degree of detachment (p < 0.001) and had a high prognostic value (the AUC was 0.8399). Determining the prognosis for not improving and deterioration 1 year after surgical treatment also had fairly high model quality indicators (AUC = 0.817 and 0.907, respectively).
регматогенне відшарування сітківки; вікова катаракта; закрита субтотальна вітректомія; факоемульсифікація; фактори ризику; прогнозування
rhegmatogenous retinal detachment; age-related cataract; closed subtotal vitrectomy; phacoemulsification; risk factors; prediction
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- D’Amico D.J. Clinical practice. Primary retinal detachment. N. Engl. J. Med. 2008. (359). 2346-2354.
- Mitry D., Charteris D.G., Fleck B.W. et al. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. Br. J. Ophthalmol. 2010. (94). 678-684.
- Colucciello M., Rasier R. Rhegmatogenous retinal detachment. Phys. Sportsmed. 2009. 37(2). 59-65.
- Poulsen C.D., Peto T., Grauslund J., Green A. Epidemiologic characteristics of retinal detachment surgery at a specialized unit in Denmark. Acta Ophthalmologica. 2016. 94(6). 548-555.
- Chen S.-N., Lian I.-B., Wei Y.-J. Epidemiology and clinical characteristics of rhegmatogenous retinal detachment in Taiwan. Bri–tish Journal of Ophthalmology. 2016. 100(9). 1216-1220.
- Mitry D., Fleck B.W., Wright A.F. et al. Pathogenesis of rhegmatogenous retinal detachment: predisposing anatomy and cell biology. Retina. 2010. (30).1561-1572.
- Sodhi A., Leung L., Do D.V. et al. Recent Trends in the Mana–gement of Rhegmatogenous Retinal Detachment. Surv. Ophthalmol. 2008. (53). 50-57.
- Park S.J., Choi N.K., Park K.H., Woo S.J. Five year nationwide incidence of rhegmatogenous retinal detachment requiring surgery in Korea. PLoS One. 2013. 8 (11). e80174.
- Warren A., Wang D.W., Lim J.I. Rhegmatogenous retinal detachment surgery: A review. Clin. Exp. Ophthalmol. 2023 Apr. 51(3). 271-279. doi: 10.1111/ceo.14205.
- Benson M.D., Sia D., Seamone M.E., Greve M., Hinz B., Tennant M.T.S. et al. Phacovitrectomy For Primary Rhegmatogenous Retinal Detachment Repair: A Retrospective Review. Retina. 2021 Apr 1. 41(4). 753-760. doi: 10.1097/IAE.0000000000002945.
- Haugstad M., Moosmayer S., Bragadόttir R. Primary rhegmato–genous retinal detachment — surgical methods and anatomical outcome. Acta Ophthalmol. 2017 May. 95(3). 247-251. doi: 10.1111/aos.13295.
- Starr M.R., Ryan E.H., Yonekawa Y. Primary Retinal Detachment Outcomes Study: summary of reports number 1 to number 18. Curr. Opin. Ophthalmol. 2023 May 1. 34(3). 211-217. doi: 10.1097/ICU.0000000000000942.
- Popovic M.M., Muni R.H., Nichani P., Kertes P.J. Pars plana vitrectomy, scleral buckle, and pneumatic retinopexy for the management of rhegmatogenous retinal detachment: a meta-analysis. Surv. Ophthalmol. 2022 Jan-Feb. 67(1). 184-196. doi: 10.1016/j.survophthal.2021.05.008.
- Гур’янов В.Г., Лях Ю.Е., Парій В.Д., Короткий Р.В., Чалий О.В., Чалий К.О., Цехмістер Я.В. Посібник з біостатистики. Аналіз результатів медичних досліджень у пакеті EZR (R-statistics). Kиїв: Вістка, 2018. 208 с.
- Hillier R.J., Felfeli T., Berger A.R., Wong D.T., Altomare F., Dai D. et al. The Pneumatic Retinopexy versus Vitrectomy for the Management of Primary Rhegmatogenous Retinal Detachment Outcomes Randomized Trial (PIVOT). Ophthalmology. 2019 Apr. 126(4). 531-539. doi: 10.1016/j.ophtha.2018.11.014.
- Haugstad M., Moosmayer S., Bragadόttir R. Primary rhegmato–genous retinal detachment — surgical methods and anatomical outcome. Acta Ophthalmol. 2017 May. 95(3). 247-251. doi: 10.1111/aos.13295.
- Sung J.Y., Lee M.W., Won Y.K., Lim H.B., Kim J.Y. Clinical characteristics and prognosis of Total Rhegmatogenous retinal detachment: a matched case-control study. BMC Ophthalmol. 2020 Jul 13. 20(1). 286. doi: 10.1186/s12886-020-01560-4.
- Wickham L., Ho-Yen G.O., Bunce C., Wong D., Charte–ris D.G. Surgical failure following primary retinal detachment surgery by vitrectomy: risk factors and functional outcomes. Br. J. Ophthalmol. 2011 Sep. 95(9). 1234-8. doi: 10.1136/bjo.2010.190306.
- Fu Y., Xie T.H., Gu Z.H., Yang N., Geng R.F., Zhang Y.L. Recurrent retinal detachment after pars plana vitrectomy with silicone oil tamponade for rhegmatogenous retinal detachment. Int. Ophthalmol. 2022 Dec. 42(12). 3813-3820. doi: 10.1007/s10792-022-02401-7.
- Kim M.S., Park J.Y., Jin K.W., Park K.H., Park S.J., Joo K., Woo S.J. Influence of Surgical Experience and Risk Factors for Surgical Failure in Primary Retinal Detachment Surgery. Ophthalmologica. 2023. 246(2). 141-149. doi: 10.1159/000530526.
- Wickham L., Bunce C., Wong D., Charteris D.G. Retinal detachment repair by vitrectomy: simplified formulae to estimate the risk of failure. Br. J. Ophthalmol. 2011 Sep. 95(9). 1239-44. doi: 10.1136/bjo.2010.190314.